Pregnancy
From Wikipedia, the free encyclopedia

| Pregnancy Classification and external resources |
|
| ICD-9 | V22 |
|---|---|
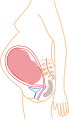
Pregnancy (latin graviditas) is the carrying of one or more offspring, known as a fetus or embryo, inside the uterus of a female. In a pregnancy, there can be multiple gestations, as in the case of twins or triplets. Human pregnancy is the most studied of all mammalian pregnancies. Obstetrics is the surgical field that studies and cares for high risk pregnancy. Midwifery is the non-surgical field that cares for pregnancy and pregnant women.
Childbirth usually occurs about 38 weeks after fertilization (conception), i.e., approximately 40 weeks from the last normal menstrual period (LNMP) in humans. The World Health Organisation defines normal term for delivery as between 37 weeks and 42 weeks. The calculation of this date involves the assumption of a regular 28-day period.
Contents |
[edit] Terminology
One scientific term for the state of pregnancy is gravid, and a pregnant female is sometimes referred to as a gravida.[1] Neither word is used in common speech. Similarly, the term "parity" (abbreviated as "para") is used for the number of previous successful live births. Medically, a woman who has never been pregnant is referred to as a "nulligravida", and in subsequent pregnancies as "multigravida" or "multiparous".[2][3][4] Hence during a second pregnancy a woman would be described as "gravida 2, para 1" and upon delivery as "gravida 2, para 2". Incomplete pregnancies of abortions, miscarriages or stillbirths account for parity values being less than the gravida number, whereas a multiple birth will increase the parity value. Women who have never carried a pregnancy achieving more than 20 weeks of gestation age are referred to as "nulliparous".[5]
The term embryo is used to describe the developing offspring during the first eight weeks following conception, and the term fetus is used from about two months of development until birth.[6][7]
In many societies' medical or legal definitions, human pregnancy is somewhat arbitrarily divided into three trimester periods, as a means to simplify reference to the different stages of prenatal development. The first trimester carries the highest risk of miscarriage (natural death of embryo or fetus). During the second trimester, the development of the fetus can be more easily monitored and diagnosed. The beginning of the third trimester often approximates the point of viability, or the ability of the fetus to survive, with or without medical help, outside of the uterus.[8]
[edit] Initiation and duration
Pregnancy occurs as the result of the female gamete or oocyte being penetrated by the male gamete spermatozoon in a process referred to, in medicine, as "fertilization", or more commonly known as "conception". After the point of "fertilization" it is referred to as an egg. The fusion of male and female gametes usually occurs through the act of sexual intercourse. However, the advent of artificial insemination and in vitro fertilisation have also made achieving pregnancy possible in cases where sexual intercourse does not result in fertilization (e.g. through choice or male/female infertility).
The expected date of delivery (EDD) is 40 weeks counting from the last menstrual period (LMP) and birth usually occurs between 37 and 42 weeks,[9] The actual pregnancy duration is typically 38 weeks after conception. Though pregnancy begins at conception, it is more convenient to date from the first day of a woman's last menstrual period, or from the date of conception if known. Starting from one of these dates, the expected date of delivery can be calculated. 40 weeks is nine months and six days, which forms the basis of Naegele's rule for estimating date of delivery. More accurate and sophisticated algorithms take into account other variables, such as whether this is the first or subsequent child (i.e. pregnant woman is a primip or a multip, respectively), ethnicity, parental age, length of menstrual cycle and menstrual regularity.
Pregnancy is considered 'at term' when gestation attains 37 complete weeks but is less than 42 (between 259 and 294 days since LMP). Events before completion of 37 weeks (259 days) are considered pre-term; from week 42 (294 days) events are considered post-term.[10] When a pregnancy exceeds 42 weeks (294 days), the risk of complications for woman and fetus increases significantly.[9][11] As such, obstetricians usually prefer to induce labour, in an uncomplicated pregnancy, at some stage between 41 and 42 weeks.[12][13]
Recent medical literature prefers the terminology pre-term and post-term to premature and post-mature. Pre-term and post-term are unambiguously defined as above, whereas premature and postmature have historical meaning and relate more to the infant's size and state of development rather than to the stage of pregnancy.[14][15]
Fewer than 5% of births occur on the due date; 50% of births are within a week of the due date, and almost 90% within two weeks.[16] It is much more useful, therefore, to consider a range of due dates, rather than one specific day, with some online due date calculators providing this information.
Accurate dating of pregnancy is important, because it is used in calculating the results of various prenatal tests (for example, in the triple test). A decision may be made to induce labour if a fetus is perceived to be overdue. Furthermore, if LMP and ultrasound dating predict different respective due dates, with the latter being later, this might signify slowed fetal growth and therefore require closer review.
[edit] Diagnosis
The beginning of pregnancy may be detected in a number of different ways, either by a pregnant woman without medical testing, or by using medical tests with or without the assistance of a medical professional.
Most pregnant women experience a number of symptoms, which can signify pregnancy. The symptoms can include nausea and vomiting, excessive tiredness and fatigue, craving for certain foods not normally considered a favorite and frequent urination particularly during night.
A number of early medical signs are associated with pregnancy.[17][18] These signs typically appear, if at all, within the first few weeks after conception. Although not all of these signs are universally present, nor are all of them diagnostic by themselves, taken together they make a presumptive diagnosis of pregnancy. These signs include the presence of human chorionic gonadotropin (hCG) in the blood and urine, missed menstrual period, implantation bleeding that occurs at implantation of the embryo in the uterus during the third or fourth week after last menstrual period, increased basal body temperature sustained for over two weeks after ovulation, Chadwick's sign (darkening of the cervix, vagina, and vulva), Goodell's sign (softening of the vaginal portion of the cervix), Hegar's sign (softening of the uterus isthmus), and pigmentation of linea alba - Linea nigra, (darkening of the skin in a midline of the abdomen, caused by hyperpigmentation resulting from hormonal changes, usually appearing around the middle of pregnancy).[17][18]
Pregnancy detection can be accomplished using one or more of various pregnancy tests which detect hormones generated by the newly-formed placenta. Clinical blood and urine tests can detect pregnancy soon after implantation, which is as early as 6-8 days after fertilization. Blood pregnancy tests are more accurate than urine tests.[19] Home pregnancy tests are personal urine tests, which normally cannot detect a pregnancy until at least 12-15 days after fertilization. Both clinical and home tests can only detect the state of pregnancy, and cannot detect the age of the embryo.
In the post-implantation phase, the blastocyst secretes a hormone named human chorionic gonadotropin which in turn, stimulates the corpus luteum in the woman's ovary to continue producing progesterone. This acts to maintain the lining of the uterus so that the embryo will continue to be nourished. The glands in the lining of the uterus will swell in response to the blastocyst, and capillaries will be stimulated to grow in that region. This allows the blastocyst to receive vital nutrients from the woman.
Despite all the signs, some women may not realize they are pregnant until they are quite far along in their pregnancy, in some cases not even until they begin labour. This can be caused by many factors, including irregular periods (quite common in teenagers), certain medications (not related to conceiving children), and obese women who disregard their weight gain. Others may be in denial of their situation.
An early sonograph can determine the age of the pregnancy fairly accurately. In practice, doctors typically express the age of a pregnancy (i.e. an "age" for an embryo) in terms of "menstrual date" based on the first day of a woman's last menstrual period, as the woman reports it. Unless a woman's recent sexual activity has been limited, or she has been charting her cycles, or the conception is as the result of some types of fertility treatment (such as IUI or IVF) the exact date of fertilization is unknown. Absent symptoms such as morning sickness, often the only visible sign of a pregnancy is an interruption of her normal monthly menstruation cycle, (i.e. a "late period"). Hence, the "menstrual date" is simply a common educated estimate for the age of a fetus, which is an average of two weeks later than the first day of the woman's last menstrual period. The term "conception date" may sometimes be used when that date is more certain, though even medical professionals can be imprecise with their use of the two distinct terms. The due date can be calculated by using Naegele's rule. The expected date of delivery may also be calculated from sonogram measurement of the fetus. This method is slightly more accurate than methods based on LMP.[20] The beginning of labour, which is variously called confinement or childbed, begins on the day predicted by LMP 3.6% of the time and on the day predicted by sonography 4.3% of the time.[21]
Diagnostic criteria are: Women who have menstrual cycles and are sexually active, a period delayed by a few days or weeks is suggestive of pregnancy; elevated B-hcG to around 100,000 mIU/mL by 10 weeks of gestation.
[edit] Physiology
- The term trimester redirects here. For the term trimester used in academic settings, see Academic term
Pregnancy is typically broken into three periods, or trimesters, each of about three months. While there are no hard and fast rules, these distinctions are useful in describing the changes that take place over time.
[edit] First trimester

Traditionally, doctors have measured pregnancy from a number of convenient points, including the day of last menstruation, ovulation, fertilization, implantation and chemical detection. In medicine, pregnancy is often defined as beginning when the developing embryo becomes implanted into the endometrial lining of a woman's uterus. In some cases where complications may have arisen, the fertilized egg might implant itself in the fallopian tubes or the cervix, causing an ectopic pregnancy. Most pregnant women do not have any specific signs or symptoms of implantation, although it is not uncommon to experience minimal bleeding at implantation. Some women will also experience cramping during their first trimester. This is usually of no concern unless there is spotting or bleeding as well. After implantation the uterine endometrium is called the decidua.The placenta which is formed partly from the decidua and partly from outer layers of the embryo is responsible for transport of nutrients and oxygen to, and removal of waste products from the fetus. The umbilical cord is the connecting cord from the embryo or fetus to the placenta.The developing embryo undergoes tremendous growth and changes during the process of foetal development.
Morning sickness can occur in about seventy percent of all pregnant women and typically improves after the first trimester.[22]
In the first 12 weeks of pregnancy the nipples and areolas darken due to a temporary increase in hormones. [23]
Most miscarriages occur during this period.

[edit] Second trimester
Months 4 through 6 of the pregnancy are called the second trimester. Most women feel more energized in this period, and begin to put on weight as the symptoms of morning sickness subside and eventually fade away.
In the 20th week the uterus, the muscular organ that holds the developing fetus, can expand up to 20 times its normal size during pregnancy. Although the fetus begins moving and takes a recognizable human shape during the first trimester, it is not until the second trimester that movement of the fetus, often referred to as "quickening", can be felt. This typically happens in the fourth month, more specifically in the 20 to 21 week, or by the 19th week if the woman has been pregnant before. However, it is not uncommon for some women to not feel the fetus move until much later. The placenta is now fully functioning and the fetus is making insulin and urinating. The reproductive organs distinguish the fetus as male or female.
[edit] Third trimester
Final weight gain takes place, which is the most weight gain throughout the pregnancy. The fetus will be growing the most rapidly during this stage, gaining up to 28g per day. The woman's belly will transform in shape as the belly drops due to the fetus turning in a downward position ready for birth. During the second trimester, the woman's belly would have been very upright, whereas in the third trimester it will drop down quite low, and the woman will be able to lift her belly up and down. The fetus begins to move regularly, and is felt by the woman. Fetal movement can become quite strong and be disruptive to the woman. The woman's navel will sometimes become convex, "popping" out, due to her expanding abdomen. This period of her pregnancy can be uncomfortable, causing symptoms like weak bladder control and back-ache. Movement of the fetus becomes stronger and more frequent and via improved brain, eye, and muscle function the fetus is prepared for ex utero viability. The woman can feel the fetus "rolling" and it may cause pain or discomfort when it is near the woman's ribs and spine.
It is during this time that a baby born prematurely may survive. The use of modern medical intensive care technology has greatly increased the probability of premature babies surviving, and has pushed back the boundary of viability to much earlier dates than would be possible without assistance.[24] In spite of these developments, premature birth remains a major threat to the fetus, and may result in ill-health in later life, even if the baby survives.
[edit] Prenatal development and sonograph images
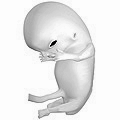
Prenatal development is divided into two primary biological stages. The first is the embryonic stage, which lasts for about two months. At this point, the fetal stage begins. At the beginning of the foetal stage, the risk of miscarriage decreases sharply,[25] all major structures including hands, feet, head, brain, and other organs are present, and they continue to grow and develop. When the fetal stage commences, a fetus is typically about 30 mm (1.2 inches) in length, and the heart can be seen beating via sonograph; the fetus bends the head, and also makes general movements and startles that involve the whole body.[26] Some fingerprint formation occurs from the beginning of the fetal stage.[27]
Electrical brain activity is first detected between the 5th and 6th week of gestation, though this is still considered primitive neural activity rather than the beginning of conscious thought, something that develops much later in fetation. Synapses begin forming at 17 weeks, and at about week 28 begin multiply at a rapid pace which continues until 3-4 months after birth. It isn't until week 23 that the fetus can survive, albeit with major medical support, outside of the womb. It is not until then that the fetus possesses a sustainable human brain. [28]
 Embryo at 4 weeks after fertilization[29] |
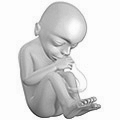
 Fetus at 8 weeks after fertilization[30] |
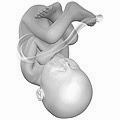
 Fetus at 18 weeks after fertilization[31] |
 Fetus at 38 weeks after fertilization[32] |
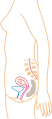 Relative size in 1st month (simplified illustration) |
 Relative size in 3rd month (simplified illustration) |
 Relative size in 5th month (simplified illustration) |
 Relative size in 9th month (simplified illustration) |
One way to observe prenatal development is via ultrasound images. Modern 3D ultrasound images provide greater detail for prenatal diagnosis than the older 2D ultrasound technology.[33] Whilst 3D is popular with parents desiring a prenatal photograph as a keepsake,[34] both 2D and 3D are discouraged by the FDA for non-medical use,[35] but there are no definitive studies linking ultrasound to any adverse medical effects.[36] The following 3D ultrasound images were taken at different stages of pregnancy:
 3-inch fetus (about 14 weeks gestational age) |
 Fetus at 17 weeks |
 Fetus at 20 weeks |
[edit] Physiological changes in pregnancy
The body must change its physiological and homeostatic mechanisms in pregnancy to ensure the fetus is provided for. Increases in blood sugar, breathing and cardiac output are all required.
[edit] Hormonal changes
Levels of progesterone and oestrogens rise continually throughout pregnancy, suppressing the hypothalamic axis and subsequently the menstrual cycle. The woman and the placenta also produce many hormones.
Prolactin levels increase due to maternal Pituitary gland enlargement by 50%. This mediates a change in the structure of the Mammary gland from ductal to lobular-alveolar. Parathyroid hormone is increased due to increases of calcium uptake in the gut and reabsorption by the kidney. Adrenal hormones such as cortisol and aldosterone also increase.
Placental lactogen is produced by the placenta and stimulates lipolysis and fatty acid metabolism by the woman, conserving blood glucose for use by the fetus. It also decreases maternal tissue sensitivity to insulin, resulting in gestational diabetes.
[edit] Musculoskeletal changes
The body's posture changes as the pregnancy progresses. The pelvis tilts and the back arches to help keep balance. Poor posture occurs naturally from the stretching of the woman's abdominal muscles as the fetus grows. These muscles are less able to contract and keep the lower back in proper alignment. The pregnant woman has a different pattern of gait. The step lengthens as the pregnancy progresses, due to weight gain and changes in posture. On average, a woman's foot can grow by a half size or more during pregnancy. In addition, the increased body weight of pregnancy, fluid retention, and weight gain lowers the arches of the foot, further adding to the foot's length and width. The influences of increased hormones such as estrogen and relaxin initiate the remodeling of soft tissues, cartilage and ligaments. Certain skeletal joints such as the symphysis pubis and sacroiliac widen or have increased laxity.
[edit] Physical changes
One of the most noticeable alterations in pregnancy is the gain in weight. The enlarging uterus, the growing fetus, the placenta and liquor amnii, the acquisition of fat and water retention, all contribute to this increase in weight. The weight gain varies from person to person and can be anywhere from 5 pounds (2.3 kg) to over 100 pounds (45 kg). In America, the doctor-recommended weight gain range is 25 pounds (11 kg) to 35 pounds (16 kg), less if the woman is overweight, more (up to 40 pounds (18 kg)) if the woman is underweight.
Other physical changes during pregnancy include breasts increasing two cup sizes. Also areas of the body such as the forehead and cheeks (known as the 'mask of pregnancy') become darker due to the increase of melanin being produced.[37]
The female body experiences many changes as the fetus grows through each trimester as shown and discussed in this pregnancy video. Two women at different stages in their pregnancy illustrate what has happened to their bodies.
[edit] Cardiovascular changes
Blood volume increases by 40% in the first two trimesters. This is due to an increase in plasma volume through increased aldosterone. Progesterone may also interact with the aldosterone receptor, thus leading to increased levels. Red blood cell numbers increase due to increased erythropoietin levels.
Cardiac function is also modified, with increase heart rate and increased stroke volume. A decrease in vagal tone and increase in sympathetic tone is the cause. Blood volume increases act to increase stroke volume of the heart via Starling's law. After pregnancy the change in stroke volume is not reversed. Cardiac output rises from 4 to 7 litres in the 2nd trimester
Blood pressure also fluctuates. In the first trimester it falls. Initially this is due to decreased sensitivity to angiotensin and vasodilation provoked by increased blood volume. Later, however, it is caused by decreased resistance to the growing uteroplacental bed.
[edit] Respiratory changes
Decreased functional residual capacity is seen, typically falling from 1.7 to 1.35 litres, due to the compression of the diaphragm by the uterus. Tidal volume increases, from 0.45 to 0.65 litres, giving an increase in pulmonary ventilation. This is necessary to meet the increased oxygen requirement of the body, which reaches 50ml/min - 20ml of which goes to reproductive tissues.
Progesterone may act centrally on chemoreceptors to reset the set point to a lower partial pressure of carbon dioxide. This maintains an increased respiration rate even at a decreased level of carbon dioxide.
[edit] Metabolic changes
An increased requirement for nutrients is given by fetal growth and fat deposition. Changes are caused by steroid hormones, lactogen and cortisol.
Maternal insulin resistance can lead to gestational diabetes. Increase liver metabolism is also seen, with increased gluconeogenesis to increase maternal glucose levels.
[edit] Renal changes
Renal plasma flow increases, as does aldosterone and erthropoietin production as discussed. The tubular maximum for glucose is reduced, which may precipitate gestational diabetes.
[edit] Management
Prenatal medical care is of recognized value throughout the developed world. Periconceptional Folic acid supplementation is the only type of supplementation of proven efficacy.
[edit] Nutrition
A balanced, nutritious diet is an important aspect of a healthy pregnancy. Eating a healthy diet, balancing carbohydrates, fat, and proteins, and eating a variety of fruits and vegetables, usually ensures good nutrition. Those whose diets are affected by health issues, religious requirements, or ethical beliefs may choose to consult a health professional for specific advice.
Adequate periconceptional folic acid (also called folate or Vitamin B9) intake has been proven to limit fetal neural tube defects, preventing spina bifida, a very serious birth defect. The neural tube develops during the first 28 days of pregnancy, explaining the necessity to guarantee adequate periconceptional folate intake.[38][39] Folates (from folia, leaf) are abundant in spinach (fresh, frozen, or canned), and are also found in green vegetables, salads, citrus fruit and melon, chickpeas (i.e. in the form of hummus or falafel), and eggs. In the United States and Canada, most wheat products (flour, noodles) are fortified with folic acid.[40]
Several micronutrients are important for the health of the developing fetus, especially in areas of the world where insufficient nutrition is prevalent.[41] In developed areas, such as Western Europe and the United States, certain nutrients such as Vitamin D and calcium, required for bone development, may require supplementation.[42][43][44]
There is some evidence that long-chain omega-3 (n-3) fatty acids have an effect on the developing fetus, but further research is required.[45] At this time, supplementing the diet with foods rich in these fatty acids is not recommended, but is not harmful.[46]
Dangerous bacteria or parasites may contaminate foods, particularly listeria and toxoplasma, toxoplasmosis agent. Careful washing of fruits and raw vegetables may remove these pathogens, as may thoroughly cooking leftovers, meat, or processed meat. Soft cheeses may contain listeria; if milk is raw the risk may increase. Cat feces pose a particular risk of toxoplasmosis. Pregnant women are also more prone to catching salmonella infections from eggs and poultry, which should be thoroughly cooked. Practicing good hygiene in the kitchen can reduce these risks.[47]
[edit] Weight gain
Caloric intake must be increased, to ensure proper development of the fetus. The amount of weight gained during pregnancy varies among women. The National Health Service recommends that overall weight gain during the 9 month period for women who start pregnancy with normal weight be 10 to 12 kilograms (22–26 lb).[48] During pregnancy, insufficient weight gain can compromise the health of the fetus. Women with fears of weight gain or with eating disorders may choose to work with a health professional, to ensure that pregnancy does not trigger disordered eating. Likewise, excessive weight gain can pose risks to the woman and the fetus. Women who are prone to being overweight may choose to plan a healthy diet and exercise to help moderate the amount of weight gained.
[edit] Immunological tolerance
Research on the immunological basis for pre-eclampsia has indicated that continued exposure to a partner's semen has a strong protective effect against pre-eclampsia, largely due to the absorption of several immune modulating factors present in seminal fluid.[49] Studies also showed that long periods of sexual cohabitation with the same partner fathering a woman's child significantly decreased her chances of suffering pre-eclampsia.[50] Several other studies have since investigated the strongly decreased incidence of pre-eclampsia in women who had received blood transfusions from their partner, those with long, preceding histories of sex without barrier contraceptives, and in women who had been regularly performing oral sex,[51] with one study concluding that "induction of allogeneic tolerance to the paternal HLA molecules of the fetus may be crucial. Data collected strongly suggests that exposure, and especially oral exposure to soluble HLA from semen can lead to transplantation tolerance."[51]
Other studies have investigated the roles of semen in the female reproductive tracts of mice, showing that "insemination elicits inflammatory changes in female reproductive tissues,"[52] concluding that the changes "likely lead to immunological priming to paternal antigens or influence pregnancy outcomes." A similar series of studies confirmed the importance of immune modulation in female mice through the absorption of specific immune factors in semen, including TGF-Beta, lack of which is also being investigated as a cause of miscarriage in women and infertility in men.
According to the theory, pre-eclampsia is frequently caused by a failure of the woman's immune system to accept the fetus and placenta, which both contain "foreign" proteins from paternal genes. Regular exposure to the father's semen causes her immune system to develop tolerance to the paternal antigens, a process which is significantly supported by as many as 93 currently identified immune regulating factors in seminal fluid.[53][54] Having already noted the importance of a woman's immunological tolerance to the fetus's paternal genes, several Dutch reproductive biologists decided to take their research a step further. Consistent with the fact that human immune systems tolerate things better when they enter the body via the mouth, the Dutch researchers conducted a series of studies that confirmed a surprisingly strong correlation between a diminished incidence of pre-eclampsia and a woman's practice of oral sex, and noted that the protective effects were strongest if she swallowed her partner's semen.[55] The researchers concluded that while any exposure to a partner's semen during sexual activity appears to decrease a woman's chances for the various immunological disorders that can occur during pregnancy, immunological tolerance could be most quickly established through oral introduction and gastrointestinal absorption of semen.[55] Recognizing that some of the studies potentially included the presence of confounding factors, such as the possibility that women who regularly perform oral sex and swallow semen might also engage in more frequent vaginal intercourse, the researchers also noted that, either way, the data still overwhelmingly supports the main theory behind all their studies--that repeated exposure to semen establishes the maternal immunological tolerance necessary for a safe and successful pregnancy.
[edit] Drugs in pregnancy
Drugs used during pregnancy can have temporary or permanent effects on the fetus. Therefore many physicians would prefer not to prescribe for pregnant women, the major concern being over teratogenicity of the drugs. This results in inappropriate treatment of pregnant women. Use of drugs in pregnancy is not always wrong. For example, high fever is harmful for the fetus in the early months. Use of paracetamol is better than no treatment at all. Also, diabetes mellitus during pregnancy may need intensive therapy with insulin. Drugs have been classified into categories A,B,C,D and X based on the Food and Drug Administration(FDA) rating system to provide therapeutic guidance based on potential benefits and fetal risks. Drugs like multivitamins that have demonstrated no fetal risks after controlled studies in humans are classified as Category A. On the other hand drugs like thalidomide with proven fetal risks that outweigh all benefits are classified as Category X.[56]
[edit] Sexuality during pregnancy
Most pregnant women can enjoy sexual intercourse throughout gravidity. Most research suggests that, during pregnancy, both sexual desire and frequency of sexual relations decrease.[57][58] In context of this overall decrease in desire, some studies indicate a second-trimester increase, preceding a decrease.[59] However, these decreases are not universal: a significant number of women report greater sexual satisfaction throughout their pregnancies.[60]
Sex during pregnancy is a low-risk behaviour except when the physician advises that sexual intercourse be avoided, which may, in some pregnancies, lead to serious pregnancy complications or health issues such as a high-risk for premature labour or a ruptured uterus. Such a decision may be based upon a history of difficulties in a previous childbirth.
Some psychological research studies in the 1980s and '90s contend that it is useful for pregnant women to continue to have sexual activity, specifically noting that overall sexual satisfaction was correlated with feeling happy about being pregnant, feeling more attractive in late pregnancy than before pregnancy and experiencing orgasm.[59] Sexual activity has also been suggested as a way to prepare for induced labour; some believe the natural prostaglandin content of seminal liquid can favour the maturation process of the cervix making it more flexible, allowing for easier and faster dilation and effacement of the cervix. However, the efficacy of using sexual intercourse as an induction agent "remains uncertain".[61]
During pregnancy, the fetus is protected from penetrative thrusting by the amniotic fluid in the womb and by the woman's cervix.[62]
After giving birth sexual intercourse can begin when the couple are both ready. However most couples wait until after six weeks and they should consult their GP if they have any concerns.[37]
[edit] Abortion
An abortion is the removal or expulsion of an embryo or fetus from the uterus, resulting in or caused by its death. This can occur spontaneously or accidentally as with a miscarriage, or be artificially induced by medical, surgical or other means.
[edit] Progression
[edit] Complaints
The following are complaints that may occur during pregnancy:
- Back pain. A particularly common complaint in the third trimester when the patient's center of gravity has shifted.
- Constipation. A complaint that is caused by decreased bowel motility secondary to elevated progesterone (normal in pregnancy), which can lead to greater absorption of water.
- Braxton Hicks contractions. Occasional, irregular, and often painless contractions that occur several times per day.
- Edema (swelling). Common complaint in advancing pregnancy. Caused by compression of the inferior vena cava (IVC) and pelvic veins by the uterus leads to increased hydrostatic pressure in lower extremities.
- Regurgitation, heartburn, and nausea. Common complaints that may be caused by Gastroesophageal Reflux Disease (GERD); this is determined by relaxation of the lower esophageal sphincter (LES) and increased transit time in the stomach (normal in pregnancy)
- Haemorrhoids. Complaint that is often noted in advancing pregnancy. Caused by increased venous stasis and IVC compression leading to congestion in venous system, along with increased abdominal pressure secondary to the pregnant space-occupying uterus and constipation.
- Pelvic girdle pain. A common complaint is pain, instability or dysfunction of the symphysis pubis and/or sacroiliac joints resulting from either excess strain or injury (such as Diastasis symphysis pubis) during the course of the pregnancy or birthing process.
- Increased urinary frequency. A common complaint referred by the gravida, caused by increased intravascular volume, elevated GFR (glomerular filtration rate), and compression of the bladder by the expanding uterus.
- Varicose veins. Common complaint caused by relaxation of the venous smooth muscle and increased intravascular pressure.
[edit] Childbirth
Childbirth is the process whereby an infant is born. It is considered by many to be the beginning of a person's life, and age is defined relative to this event in most cultures.
A woman is considered to be in labour when she begins experiencing regular uterine contractions, accompanied by changes of her cervix — primarily effacement and dilation. While childbirth is widely experienced as painful, some women do report painless labours, while others find that concentrating on the birth helps to quicken labour and lessen the sensations. Most births are successful vaginal births, but sometimes complications arise and a woman may undergo a caesarean section.
During the time immediately after birth, both the mother and the baby are hormonally cued to bond, the mother through the release of oxytocin, a hormone also released during breastfeeding.
[edit] Postnatal period
[edit] Context
There are fine distinctions between the concepts of fertilization and the actual state of pregnancy, which starts with implantation. In a normal pregnancy, the fertilization of the egg usually will have occurred in the Fallopian tubes or in the uterus. (Often, an egg may become fertilized yet fail to become implanted in the uterus.) If the pregnancy is the result of in-vitro fertilization, the fertilization will have occurred in a Petri dish, after which pregnancy begins when one or more zygotes implant after being transferred by a physician into the woman's uterus.
In the context of political debates regarding a proper definition of life, the terminology of pregnancy can be confusing. The medically and politically neutral term which remains is simply "pregnancy," though this can be problematic as it only refers indirectly to the embryo or fetus. De Crespigny observes that doctors' language has a powerful influence over the way patients think, and thus proposes that the best interests of patients are served by using language that both supports patient autonomy and is neutral.[63]
[edit] See also
[edit] References
- ^ "Definition of gravida". The Free Dictionary/Medical Dictionary. Farlex, Inc. http://medical-dictionary.thefreedictionary.com/gravida. Retrieved on 2008-01-17.
- ^ "Definition of gravida". The Free Dictionary. Farlex, Inc. http://www.thefreedictionary.com/gravida. Retrieved on 2008-01-17.
- ^ [medical-dictionary.thefreedictionary.com/nulligravida The American Heritage Medical Dictionary Copyright] (definition of nulligravida).
- ^ Merriam-Webster's Medical Dictionary (definition of nulligravida).
- ^ "Nulliparous Definition". MedicineNet.com. MedicineNet, Inc. http://www.medterms.com/script/main/art.asp?articlekey=15259. Retrieved on 2008-01-17.
- ^ "Embryo Definition". MedicineNet.com. MedicineNet, Inc. http://www.medterms.com/script/main/art.asp?articlekey=3225. Retrieved on 2008-01-17.
- ^ "Fetus Definition". MedicineNet.com. MedicineNet, Inc. http://www.medterms.com/script/main/art.asp?articlekey=3424. Retrieved on 2008-01-17.
- ^ "Trimester Definition". MedicineNet.com. MedicineNet, Inc. http://www.medterms.com/script/main/art.asp?articlekey=11446. Retrieved on 2008-01-17.
- ^ a b Norwitz, MD, PhD, Errol R (September 2007). "Patient information: Postterm pregnancy". UpToDate. UpToDate, inc.. http://patients.uptodate.com/topic.asp?file=pregnan/5708. Retrieved on 2008-01-16.
- ^ "Definitions". Saskatchewan Prevention Institute.. http://www.preventioninstitute.sk.ca/home/Program_Areas/Maternal__Infant_Health/Definitions/. Retrieved on 2008-01-16.
- ^ The American College of Obstetricians and Gynecologists (April 2006). "What To Expect After Your Due Date". Medem. Medem, Inc.. http://www.medem.com/MedLB/article_detaillb.cfm?article_ID=ZZZRDLPH97C&sub_cat=2005. Retrieved on 2008-01-16.
- ^ Royal College of Obstetricians and Gynaecologists (2001). "Royal College of Obstetricians and Gynaecologists Induction of labour Evidence based Guideline" (PDF). Royal College of Obstetricians and Gynaecologists. Royal College of Obstetricians and Gynaecologists. http://www.rcog.org.uk/resources/public/pdf/rcog_induction_of_labour.pdf. Retrieved on 2008-01-18.
- ^ Stovall, M.D., Thomas G. (2004-03-23). "Postdate Pregnancy". Durham Obstetrics and Gynecology. Durham Obstetrics and Gynecology. http://www.durhamobgyn.com/viewArticle?ID=336380. Retrieved on 2008-01-18.
- ^ "Definition of Premature birth". Medicine.net. http://www.medterms.com/script/main/art.asp?articlekey=11895. Retrieved on 2008-01-16.
- ^ Lama Rimawi, MD (2006-09-22). "Premature Infant". Disease & Conditions Encyclopedia. Discovery Communications, LLC.. http://health.discovery.com/encyclopedias/illnesses.html?article=2728. Retrieved on 2008-01-16.
- ^ Dr Sally Tracy, Having a Great Birth in Australia ed. David Vernon, Australian College of Midwives, 2005, p22
- ^ a b "Early symptoms of pregnancy: What happens right away". Mayo Clinic. February 22, 2007. http://www.mayoclinic.com/health/symptoms-of-pregnancy/PR00102. Retrieved on 2007-08-22.
- ^ a b "Pregnancy Symptoms - Early Signs of Pregnancy : American Pregnancy Association". http://www.americanpregnancy.org/gettingpregnant/earlypregnancysymptoms.html. Retrieved on 2008-01-16.
- ^ "BestBets: Serum or Urine beta-hCG?". http://www.bestbets.org/bets/bet.php?id=936.
- ^ Nguyen, T.H.; et al. (1999). "Evaluation of ultrasound-estimated date of delivery in 17 450 spontaneous singleton births: do we need to modify Naegele's rule?" (abstract). Ultrasound in Obstetrics and Gynecology 14 (1): 23–28. doi:. http://www.blackwell-synergy.com/doi/abs/10.1046/j.1469-0705.1999.14010023.x. Retrieved on 2007-08-18.
- ^ Odutayo, Rotimi; Odunsi, Kunle (n.d.). "Post Term Pregnancy". http://hygeia.org/poems23.htm. Retrieved on 2007-08-18.
- ^ Early pregnancy: Morning sickness, fatigue and other common symptoms
- ^ "Pregnancy video". Channel 4. 2008. http://sexperienceuk.channel4.com/education/about/pregnancy. Retrieved on 2009-01-22.
- ^ Iams JD; Romero R, Culhane JF, Goldenberg RL (12 January 2008). "Primary, secondary, and tertiary interventions to reduce the morbidity and mortality of preterm birth". Lancet 371 (9607): 164–75. doi:. PMID 18191687.
- ^ • Q&A: Miscarriage. (August 6 , 2002). BBC News. Retrieved 2007-04-22: “The risk of miscarriage lessens as the pregnancy progresses. It decreases dramatically after the 8th week.”
• Lennart Nilsson, A Child is Born 91 (1990): at eight weeks, "the danger of a miscarriage … diminishes sharply."
• “Women’s Health Information”, Hearthstone Communications Limited: “The risk of miscarriage decreases dramatically after the 8th week as the weeks go by.” Retrieved 2007-04-22. - ^ Prechtl, Heinz. "Prenatal and Early Postnatal Development of Human Motor Behavior" in Handbook of brain and behaviour in human development, Kalverboer and Gramsbergen eds., pp. 415-418 (2001 Kluwer Academic Publishers). Retrieved 2007-03-04.
- ^ Zabinski, Mark. Forensic Series Seminar, Pastore Chemical Laboratory, University of Rhode Island (February 2003) (news report retrieved 2007-01-20).
- ^ Illes, Judy. Neuroethics: Defining the Issues in Theory, Practice, and Policy (Oxford University Press 2006): "The first sign of electrical brain activity occurs at the end of week 5 and the beginning of week 6 (Brody 1975). This is far from the beginning of conscious brain activity; it is primitive neural activity. [...] synapses start forming during week 17 and multiply rapidly around week 28, continuing at a rapid pace up until 3-4 months after birth. However, despite all this amazing and rapid growth and development, it is not until week 23 that the fetus can survive, with major medical support, outside of the womb. Before this, the fetus is simply laying the foundations for a brain--a very different thing from having a sustainable human brain." Retrieved 2008-12-11.
- ^ 3D Pregnancy (Image from gestational age of 6 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here, and a sketch is available here.
- ^ 3D Pregnancy (Image from gestational age of 10 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here, and a sketch is available here.
- ^ 3D Pregnancy (Image from gestational age of 20 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here, and a sketch is available here.
- ^ 3D Pregnancy (Image from gestational age of 40 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here, and a sketch is available here.
- ^ Dimitrova V, Markov D, Dimitrov R (2007). "[3D and 4D ultrasonography in obstetrics]" (in Bulgarian). Akush Ginekol (Sofiia) 46 (2): 31–40. PMID 17469450.
- ^ Sheiner E, Hackmon R, Shoham-Vardi I, et al (2007). "A comparison between acoustic output indices in 2D and 3D/4D ultrasound in obstetrics". Ultrasound Obstet Gynecol 29 (3): 326–8. doi:. PMID 17265534.
- ^ Rados C (January-February 2004). "FDA Cautions Against Ultrasound 'Keepsake' Images". FDA Consumer Magazine. http://www.fda.gov/FDAC/features/2004/104_images.html.
- ^ Kempley R (2003-08-09). "The Grin Before They Bear It; Peek-a-Boo: Prenatal Portraits for the Ultrasound Set". Washington Post. http://www.highbeam.com/doc/1P2-279063.html.
- ^ a b "Pregnancy video". Channel 4. 2008. http://sexperienceuk.channel4.com/education/about/pregnancy. Retrieved on 2009-01-22.
- ^ Klusmann A, Heinrich B, Stöpler H, Gärtner J, Mayatepek E, Von Kries R (2005). "A decreasing rate of neural tube defects following the recommendations for periconceptional folic acid supplementation". Acta Paediatr. 94 (11): 1538–42. doi:. PMID 16303691. http://www.blackwell-synergy.com/openurl?genre=article&sid=nlm:pubmed&issn=0803-5253&date=2005&volume=94&issue=11&spage=1538. Retrieved on 2008-01-20.
- ^ Stevenson RE, Allen WP, Pai GS, Best R, Seaver LH, Dean J, Thompson S (2000). "Decline in prevalence of neural tube defects in a high-risk region of the United States". Pediatrics 106 (4): 677–83. doi:. PMID 11015508.
- ^ "Use of supplements containing folic acid among women of childbearing age--United States, 2007". MMWR Morb. Mortal. Wkly. Rep. 57 (1): 5–8. 2008. PMID 18185493.
- ^ Haider BA, Bhutta ZA (2006). "Multiple-micronutrient supplementation for women during pregnancy". Cochrane Database Syst Rev (4): CD004905. doi:. PMID 17054223.
- ^ Theobald HE (2007). "Eating for pregnancy and breast-feeding". J Fam Health Care 17 (2): 45–9. PMID 17476978.
- ^ Basile LA, Taylor SN, Wagner CL, Quinones L, Hollis BW (2007). "Neonatal vitamin D status at birth at latitude 32 degrees 72': evidence of deficiency". J Perinatol 27 (9): 568–71. doi:. PMID 17625571.
- ^ Kuoppala T, Tuimala R, Parviainen M, Koskinen T, Ala-Houhala M (1986). "Serum levels of vitamin D metabolites, calcium, phosphorus, magnesium and alkaline phosphatase in Finnish women throughout pregnancy and in cord serum at delivery". Hum Nutr Clin Nutr 40 (4): 287–93. PMID 3488981.
- ^ Hösli I, Zanetti-Daellenbach R, Holzgreve W, Lapaire O (2007). "Role of omega 3-fatty acids and multivitamins in gestation" (abstract). J Perinat Med 35 Suppl 1: S19–24. doi:. PMID 17302536. http://www.extenza-eps.com/doi/abs/10.1515/JPM.2007.032. Retrieved on 2008-01-20.
- ^ Dubnov-Raz G, Finkelstein Y, Koren G (2007). "Omega-3 fatty acid supplementation during pregnancy: for mother, baby, or neither?". Can Fam Physician 53 (5): 817–8. PMID 17872742. http://www.cfp.ca/cgi/pmidlookup?view=long&pmid=17872742. Retrieved on 2008-01-20.
- ^ Tarlow MJ (August 1994). "Epidemiology of neonatal infections". J Antimicrob Chemother 34 (Suppl A): 43–52. doi:. PMID 7844073.
- ^ How much weight will I put on during my pregnancy?
- ^ Sarah Robertson. "Research Goals". http://www.health.adelaide.edu.au/og/people/staff/robertsons.html.
- ^ Einarsson, Jon I. MD; Sangi-Haghpeykar, Haleh PhD; Gardner, Michael O. MD, MPH (2003). "Sperm exposure and development of preeclampsia". Journal of Obstetrics and Gynecology 188 (5): 1241–1243. doi:.
- ^ a b Koelman CA, Coumans AB, Nijman HW, Doxiadis II, Dekker GA, Claas FH (2000). "Correlation between oral sex and a low incidence of preeclampsia: a role for soluble HLA in seminal fluid?". J. Reprod. Immunol. 46 (2): 155–66. doi:. PMID 10706945.
- ^ Martina Johansson, John J Bromfield, Melinda J Jasper, and Sarah A Robertson (2004). "Semen activates the female immune response during early pregnancy in mice". Journal of Immunology 112 (2): 290–300. doi:.
- ^ Burne, Jerome (2006-01-30). "Give Sperm a Fighting Chance". The Times.
- ^ "Sex Primes Women for Sperm". BBC News. 2002-02-06.
- ^ a b Fox, Douglas (2002-02-09). "Gentle Persuasion". The New Scientist.
- ^ Powerpoint on Drugs in Pregnancy & Teratogenicity,Reena Shaji,MD.Obstetrics & Gynecology
- ^ M.P. Bermudez; A.I. Sanchez, G. Buela-Casal (2001). "Influence of the Gestation Period on Sexual Desire". Psychology in Spain 5 (1): 14–16.
- ^ Wing Yee Fok; Louis Yik-Si Chan, Pong Mo Yuen (10 2005). "Sexual behavior and activity in Chinese pregnant women". Acta Obstetricia et Gynecologica Scandinavica 84 (10): 934–938. doi:. PMID 16167907.
- ^ a b Reamy K; White SE, Daniell WC, Le Vine ES (June 1982). "Sexuality and pregnancy. A prospective study". J Reprod Med. 27 (6): 321–7. PMID 7120209.
- ^ Khamis MA; Mustafa MF, Mohamed SN, Toson MM (2007). "Influence of gestational period on sexual behavior". J Egypt Public Health Assoc. 2007 82 (1-2): 65–90. PMID 18217325.
- ^ Methods for Cervical Ripening and Induction of Labor - May 15, 2003 - American Family Physician
- ^ The Joy of Sex During Pregnancy - March of Dimes
- ^ de Crespigny L. (March 2003). "Words matter: nomenclature and communication in perinatal medicine". Clin Perinatol 30 (1): 17–25. doi:. PMID 12696783.
[edit] External links
- Genesis: In the womb- Slideshow
| Wikimedia Commons has media related to: Pregnancy |
|
|||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

