Shallow water blackout
From Wikipedia, the free encyclopedia
A shallow water blackout is a loss of consciousness caused by cerebral hypoxia towards the end of a breath-hold dive in water typically shallower than five metres (16 feet), when the swimmer does not necessarily experience an urgent need to breathe and has no other obvious medical condition that might have caused it.[1][2][3] Victims are often established practitioners of breath-hold diving, are fit, strong swimmers, and have not experienced problems before.
Many drowning and near drowning events occur among swimmers who black out underwater while free-diving or doing breath-hold pool laps. Blacking out, or browning out, near the end of a breath-hold dive is common. Although the mechanism is well understood, it is not common knowledge among breath-hold divers.
Shallow water blackout is related to, but differs from deep water blackout in its characteristics, mechanism and prevention; deep water blackout is precipitated by depressurisation on ascent from depth.[3][4] Blackout may also be referred to as a syncope or fainting.
Contents |
[edit] The role of hyperventilation

Otherwise unexplained blackouts underwater have been associated with the practice of hyperventilation.[1][2][3][5] Survivors of shallow water blackouts often report using hyperventilation as a technique to increase the time they can spend underwater. Hyperventilation, or over-breathing, involves breathing faster and deeper than the body naturally demands and is often used by divers in the mistaken belief that this will increase oxygen (O2) saturation. Although this appears true intuitively, the breathing rate dictated by the body alone is sufficient, even during quite strenuous activity, to ensure that the body is saturated with as much O2 as is necessary. What is really happening differs from divers' understanding; these divers are extending their dive by closing down the body's natural breathing mechanism, not by increasing oxygen load. The mechanism is as follows:
The primary urge to breathe is triggered by rising carbon dioxide (CO2) levels in the bloodstream.[5] CO2 builds up in the bloodstream when O2 is metabolized and it needs to be expelled as a waste product. The body detects CO2 levels very accurately and relies on this to control breathing.[5] Hyperventilation artificially depletes this (CO2) causing a low blood carbon dioxide condition called hypocapnia. Hypocapnia reduces the reflexive respiratory drive, allows the delay of breathing and leaves the diver susceptible to loss of consciousness from hypoxia. Although the body is able to detect low oxygen levels for most healthy people the first sign of low O2 is a brownout or unconsciousness; there is no bodily sensation that warns a diver of an impending blackout.
Significantly, victims drown quietly underwater without alerting anyone to the fact that there is a problem and are typically found on the bottom as shown in the image right. Pool lifesavers are trained to scan the bottom for the situation shown.
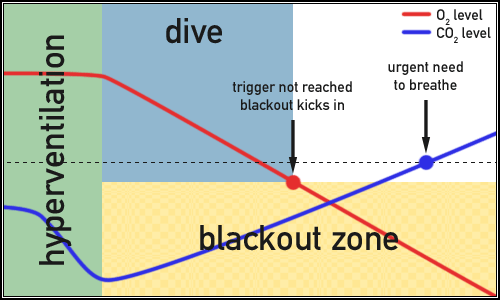
The diagram below shows the O2 and CO2 levels in the blood over the duration of a safe dive. Prior to the dive the green area shows the stabilisation of O2 and CO2 through normal breathing. The dive ends safely when the diver is forced to the surface by an urgent need to breathe.

In the next diagram hyperventilation prior to the dive has artificially depressed CO2 levels without elevating the O2 level. This pre-dive state is hence likely to result in shallow water blackout. Now note how the O2 level drops into the diver's blackout zone before the CO2 can rise enough to force the diver to resurface to breathe. The dive is extended a little, but this diver may not survive.
Breath-hold divers who hyperventilate before a dive are at risk of drowning. Many drownings unattributed to any other cause result from shallow water blackout and could be avoided if this mechanism was properly understood and the practice eliminated. Hyperventilation does not increase diving time by any notable amount. Shallow water blackout can be avoided by ensuring that carbon dioxide levels in the body are properly calibrated prior to diving and that appropriate safety measures are in place; this can be achieved if divers do the following:
- Take a moment on the edge of the water to relax and allow blood oxygen and carbon dioxide to reach equilibrium.
- Breathe absolutely normally; allow the body to dictate the rate of breathing to make sure the carbon dioxide levels are properly calibrated.
- If excited or anxious about the dive take extra care to remain calm and breathe naturally; epinephrine (adrenaline) also causes hyperventilation without the diver knowing.
- When the urge to breathe comes on near the end of the dive immediately seek access to air.
- Never pre-ventilate using blended gas mixtures such as Nitrox, Trimix or Heliair that might purge carbon dioxide in a bid to extend the dive.
- Never dive alone. Dive in buddy pairs, one to observe, one to dive.
- Buddy pairs must both know cardiopulmonary resuscitation (CPR) current practice.
Excessive hypocapnia is readily identifiable as it causes dizziness and tingling of the fingers, refer to hyperventilation for details. Conservative breathe-hold divers who hyperventilate but stop doing so before the onset of these symptoms are likely already hypocapnic without knowing it. These extreme symptoms are caused by the increase of blood pH (alkalosis) following the reduction of CO2, which is required to maintain the acidity of the blood. The absence of any symptoms of hypocapnia is not an indication that the diver’s CO2 is properly calibrated and cannot be taken as an indication that it is therefore safe to dive.
Note that the body can actually detect low levels of oxygen but that this is not normal. Persistently elevated levels of carbon dioxide in the blood, hypercapnia (the opposite to hypocapnia), tend to desensitise the body to CO2, in which case the body may come to rely on the oxygen level in the blood to maintain respiratory drive. This is illustrated in the scenario of type II respiratory failure. However, in a normal healthy person there is no subjective awareness of low oxygen levels.
Shallow water blackout should be considered alongside deep water blackout.
[edit] Deep water blackout
The mechanism for deep water blackout differs from that for shallow water blackouts and does not necessarily follow hyperventilation.[3][4] However, hyperventilation will exacerbate it and the two should be considered together. Shallow water blackouts can happen in extremely shallow water; brownouts can be induced even on dry land following hyperventilation and apnoea. However, the effect becomes much more dangerous in the ascent stage of a deep free dive. Refer to deep water blackout for more detail. There is considerable confusion surrounding the terms shallow and deep water blackout and they are made to refer to different things, or used interchangeably, in different water sports circles. For the purposes of this article the two are separate phenomena with the following characteristics:
Deep water blackout occurs as the surface is approached following a breathe-hold dive of over ten metres and typically involves deep, free-divers practicing dynamic apnoea depth diving usually at sea.[4] The immediate cause of deep water blackout is the rapid drop in the partial pressure of oxygen in the lungs on ascent.
Shallow water blackout only occurs where all phases of the dive have taken place in shallow water where depressurization is not a factor and typically involves dynamic apnoea distance swimmers, usually in a swimming pool.[3] The primary mechanism for shallow water blackout is hypocapnia brought about by hyperventilation prior to the dive.
[edit] See also
- Deep water blackout, for more on this closely related topic.
- Drowning, for more on the mechanism and physiology of drowning.
- Cheyne-Stokes respiration, another condition involving oxygen / carbon dioxide imbalance and which can affect healthy mountaineers.
- Free-diving, for more on the practice of breath-hold diving as a sport.
[edit] References
- ^ a b Brubakk, A. O.; T. S. Neuman (2003). Bennett and Elliott's physiology and medicine of diving, 5th Rev ed.. United States: Saunders Ltd.. p. 800. ISBN 0702025712.
- ^ a b Lindholm P, Pollock NW, Lundgren CEG, eds. (2006). Breath-hold diving. Proceedings of the Undersea and Hyperbaric Medical Society/Divers Alert Network 2006 June 20-21 Workshop.. Durham, NC: Divers Alert Network. ISBN 978-1-930536-36-4. http://archive.rubicon-foundation.org/5612. Retrieved on 2008-07-21.
- ^ a b c d e Edmonds, C (1968). "Shallow Water Blackout.". Royal Australian Navy, School of Underwater Medicine. RANSUM-8-68. http://archive.rubicon-foundation.org/4954. Retrieved on 2008-07-21.
- ^ a b c Elliott, D (1996). "Deep Water Blackout.". South Pacific Underwater Medicine Society journal 26 (3). ISSN 0813-1988. OCLC 16986801. http://archive.rubicon-foundation.org/6311. Retrieved on 2008-07-21.
- ^ a b c Lindholm P, Lundgren CE (2006). "Alveolar gas composition before and after maximal breath-holds in competitive divers". Undersea Hyperb Med 33 (6): 463–7. PMID 17274316. http://archive.rubicon-foundation.org/5053. Retrieved on 2008-07-21.
[edit] Additional reading
- Lindholm P (April 2007). "Loss of motor control and/or loss of consciousness during breath-hold competitions". Int J Sports Med 28 (4): 295–9. doi:. PMID 17024640. http://www.thieme-connect.com/DOI/DOI?10.1055/s-2006-924361. Retrieved on 2008-07-21.
- NW Pollock, RD Vann, ED Thalmann and CE Lundgren. (1997). "Oxygen-Enhanced Breath-hold Diving, Phase I: Hyperventilation and Carbon Dioxide Elimination.". In: EJ Maney, Jr and CH Ellis, Jr (Eds.) Diving for Science...1997. Proceedings of the American Academy of Underwater Sciences (17th Annual Scientific Diving Symposium). http://archive.rubicon-foundation.org/4647. Retrieved on 2008-07-21.
[edit] External links
- Apnea Academy - for resources on underwater apnea
- Apnea Magazine - news and articles on underwater apnea
- Aquatic Safety Research Group – excellent resources and further links
- Dying for Air - example by Walter Griffiths, M.D. and Tom Griffiths, Ed.D. in Aquatics International 2005
- Shallow-Water Blackout is No Joke - Lt. Douglas Chandler, Naval Safety Centre
- Shallow Water Blackout - Naval Safety Centre
- Swimmer Discovers Dangers of Water Blackout - Lifesaving Resources Inc. for interesting personal perspective
- Shallow Water Death - Maj. James Law in the Combat Edge 2003
- Shallow Water Blackout - Dr. Scott Duke in YMCA SCUBA Currents
- The Dangers of Underwater Swimming Are Real - Bruce Wigo in ASCA Online
- Scubadoc's Diving Medicine Online: Latent Hypoxia

