Psoriasis
From Wikipedia, the free encyclopedia
| Psoriasis Classification and external resources |
|
 |
|
|---|---|
| A person whose back and arms are affected by psoriasis | |
| ICD-10 | L40. |
| ICD-9 | 696 |
| OMIM | 177900 |
| DiseasesDB | 10895 |
| MedlinePlus | 000434 |
| eMedicine | emerg/489 Dermatology:derm/365 plaque derm/361 guttate derm/363 nails derm/366 pustular Arthritis derm/918 Radiology radio/578 Physical Medicine pmr/120 |
| MeSH | D011565 |
Psoriasis (pronounced /səˈraɪəsɪs/) is a chronic, non-contagious autoimmune disease which affects the skin and joints. It commonly causes red scaly patches to appear on the skin. The scaly patches caused by psoriasis, called psoriatic plaques, are areas of inflammation and excessive skin production. Skin rapidly accumulates at these sites and takes on a silvery-white appearance. Plaques frequently occur on the skin of the elbows and knees, but can affect any area including the scalp and genitals. In contrast to eczema, psoriasis is more likely to be found on the extensor aspect of the joint.
The disorder is a chronic recurring condition which varies in severity from minor localized patches to complete body coverage. Fingernails and toenails are frequently affected (psoriatic nail dystrophy) and can be seen as an isolated finding. Psoriasis can also cause inflammation of the joints, which is known as psoriatic arthritis. Ten to fifteen percent of people with psoriasis have psoriatic arthritis.
The cause of psoriasis is not known, but it is believed to have a genetic component. Factors that may aggravate psoriasis include stress, excessive alcohol consumption, and smoking.[1] There are many treatments available, but because of its chronic recurrent nature psoriasis is a challenge to treat.
Contents |
[edit] History
Psoriasis is probably one of the longest known illnesses of humans and simultaneously one of the most misunderstood. Some scholars believe psoriasis to have been included among the skin conditions called tzaraat in the Bible.[2] In more recent times psoriasis was frequently described as a variety of leprosy. The Greeks used the term lepra (λεπρα) for scaly skin conditions. They used the term psora to describe itchy skin conditions. It became known as Willan's lepra in the late 18th century when English dermatologists Robert Willan and Thomas Bateman differentiated it from other skin diseases. They assigned names to the condition based on the appearance of lesions. Willan identified two categories: leprosa graecorum and psora leprosa.
While it may have been visually, and later semantically, confused with leprosy, it was not until 1841 that the condition was finally given the name psoriasis by the Viennese dermatologist Ferdinand von Hebra. The name is derived from the Greek word psora which means to itch.[3]
In Ayurveda, the herbal system of India, a condition which clinically resembles psoriasis was described in sources that historians believe date from the first or second centuries AD.[citation needed]
It was during the 20th century that psoriasis was further differentiated into specific types.
[edit] Types

The symptoms of psoriasis can manifest in a variety of forms. Variants include plaque, pustular, guttate and flexural psoriasis. This section describes each type (with ICD-10 code [5]).[4]
Plaque psoriasis (psoriasis vulgaris) (L40.0) is the most common form of psoriasis. It affects 80 to 90% of people with psoriasis. Plaque psoriasis typically appears as raised areas of inflamed skin covered with silvery white scaly skin. These areas are called plaques.
Flexural psoriasis (inverse psoriasis) (L40.83-4) appears as smooth inflamed patches of skin. It occurs in skin folds, particularly around the genitals (between the thigh and groin), the armpits, under an overweight stomach (pannus), and under the breasts (inframammary fold). It is aggravated by friction and sweat, and is vulnerable to fungal infections.
Guttate psoriasis (L40.4) is characterized by numerous small round spots (differential diagnosis—pityriasis rosea—oval shape lesion). These numerous spots of psoriasis appear over large areas of the body, such as the trunk, limbs, and scalp. Guttate psoriasis is associated with streptococcal throat infection.
Pustular psoriasis (L40.1-3, L40.82) appears as raised bumps that are filled with non-infectious pus (pustules). The skin under and surrounding the pustules is red and tender. Pustular psoriasis can be localised, commonly to the hands and feet (palmoplantar pustulosis), or generalised with widespread patches occurring randomly on any part of the body.

Nail psoriasis (L40.86) produces a variety of changes in the appearance of finger and toe nails. These changes include discolouring under the nail plate, pitting of the nails, lines going across the nails, thickening of the skin under the nail, and the loosening (onycholysis) and crumbling of the nail.
Psoriatic arthritis (L40.5) involves joint and connective tissue inflammation. Psoriatic arthritis can affect any joint but is most common in the joints of the fingers and toes. This can result in a sausage-shaped swelling of the fingers and toes known as dactylitis. Psoriatic arthritis can also affect the hips, knees and spine (spondylitis). About 10-15% of people who have psoriasis also have psoriatic arthritis.[citation needed]
Erythrodermic psoriasis (L40.85) involves the widespread inflammation and exfoliation of the skin over most of the body surface. It may be accompanied by severe itching, swelling and pain. It is often the result of an exacerbation of unstable plaque psoriasis, particularly following the abrupt withdrawal of systemic treatment. This form of psoriasis can be fatal, as the extreme inflammation and exfoliation disrupt the body's ability to regulate temperature and for the skin to perform barrier functions.[5]
[edit] Clinical classification
Psoriasis is a chronic relapsing disease of the skin, which may be classified into nonpustular and pustular types as follows[6]:
- Nonpustular psoriasis
- Psoriasis vulgaris (Chronic stationary psoriasis, Plaque-like psoriasis)
- Psoriatic erythroderma (Erythrodermic psoriasis)
- Pustular psoriasis
- Generalized pustular psoriasis (Pustular psoriasis of von Zumbusch)
- Pustulosis palmaris et plantaris (Persistent palmoplantar pustulosis, Pustular psoriasis of the Barber type, Pustular psoriasis of the extremities)
- Annular pustular psoriasis
- Acrodermatitis continua
- Impetigo herpetiformis
Additional types of psoriasis include[7]:
[edit] Diagnosis
A diagnosis of psoriasis is usually based on the appearance of the skin. There are no special blood tests or diagnostic procedures for psoriasis. Sometimes a skin biopsy, or scraping, may be needed to rule out other disorders and to confirm the diagnosis. Skin from a biopsy will show clubbed Rete pegs if positive for psoriasis. Another sign of psoriasis is that when the plaques are scraped, one can see pinpoint bleeding from the skin below (Auspitz's sign).

[edit] Severity
Psoriasis is usually graded as mild (affecting less than 3% of the body), moderate (affecting 3-10% of the body) or severe.[citation needed] Several scales exist for measuring the severity of psoriasis. The degree of severity is generally based on the following factors: the proportion of body surface area affected; disease activity (degree of plaque redness, thickness and scaling); response to previous therapies; and the impact of the disease on the person.
The Psoriasis Area Severity Index (PASI) is the most widely used measurement tool for psoriasis. PASI combines the assessment of the severity of lesions and the area affected into a single score in the range 0 (no disease) to 72 (maximal disease).[8] Nevertheless, the PASI can be too unwieldy to use outside of trials, which has led to attempts to simplify the index for clinical use.[9]
[edit] Effect on the quality of life
|
|
This section does not cite any references or sources. Please help improve this article by adding citations to reliable sources (ideally, using inline citations). Unsourced material may be challenged and removed. (October 2008) |
Psoriasis has been shown to affect health-related quality of life to an extent similar to the effects of other chronic diseases such as depression, myocardial infarction, hypertension, congestive heart failure or type 2 diabetes. Depending on the severity and location of outbreaks, individuals may experience significant physical discomfort and some disability. Itching and pain can interfere with basic functions, such as self-care, walking, and sleep. Plaques on hands and feet can prevent individuals from working at certain occupations, playing some sports, and caring for family members or a home. Plaques on the scalp can be particularly embarrassing as flaky plaque in the hair can be mistaken for dandruff. The frequency of medical care is costly and can interfere with an employment or school schedule.
Individuals with psoriasis may also feel self-conscious about their appearance and have a poor self-image that stems from fear of public rejection and psychosexual concerns. Psychological distress can lead to significant depression and social isolation.
In a 2008 National Psoriasis Foundation survey of 426 psoriasis sufferers, 71 percent reported that the disease was a significant problem in everyday life. More than half reported significant feelings of self-consciousness (63 percent) and embarrassment (58 percent). More than one-third said they avoided social activities and limited dating or intimate interactions.[10]
[edit] Epidemiology
Psoriasis affects both sexes equally and can occur at any age, although it most commonly appears for the first time between the ages of 15 and 25 years.
The prevalence of psoriasis in Western populations is estimated to be around 2-3%. The prevalence of psoriasis among 7.5 million patients who were registered with a general practitioner in the United Kingdom was 1.5%.[11] A survey[12] conducted by the National Psoriasis Foundation (a US based psoriasis education and advocacy group) found a prevalence of 2.1% among adult Americans. The study found that 35% of people with psoriasis could be classified as having moderate to severe psoriasis.
Around one-third of people with psoriasis report a family history of the disease, and researchers have identified genetic loci associated with the condition. Studies of monozygotic twins suggest a 70% chance of a twin developing psoriasis if the other twin has psoriasis. The concordance is around 20% for dizygotic twins. These findings suggest both a genetic predisposition and an environmental response in developing psoriasis.[13]
Onset before age 40 usually indicates a greater genetic susceptibility and a more severe or recurrent course of psoriasis.
[edit] Cause
The cause of psoriasis is not fully understood. There are two main hypotheses about the process that occurs in the development of the disease. The first considers psoriasis as primarily a disorder of excessive growth and reproduction of skin cells. The problem is simply seen as a fault of the epidermis and its keratinocytes. The second hypothesis sees the disease as being an immune-mediated disorder in which the excessive reproduction of skin cells is secondary to factors produced by the immune system. T cells (which normally help protect the body against infection) become active, migrate to the dermis and trigger the release of cytokines (tumor necrosis factor-alpha TNFα, in particular) which cause inflammation and the rapid production of skin cells. It is not known what initiates the activation of the T cells.
The immune-mediated model of psoriasis has been supported by the observation that immunosuppressant medications can clear psoriasis plaques. However, the role of the immune system is not fully understood, and it has recently been reported that an animal model of psoriasis can be triggered in mice lacking T cells.[14] Animal models, however, reveal only a few aspects resembling human psoriasis.
Psoriasis is a fairly idiosyncratic disease. The majority of people's experience of psoriasis is one in which it may worsen or improve for no apparent reason. Studies of the factors associated with psoriasis tend to be based on small (usually hospital based) samples of individuals. These studies tend to suffer from representative issues, and an inability to tease out causal associations in the face of other (possibly unknown) intervening factors. Conflicting findings are often reported. Nevertheless, the first outbreak is sometimes reported following stress (physical and mental), skin injury, and streptococcal infection. Conditions that have been reported as accompanying a worsening of the disease include infections, stress, and changes in season and climate. Certain medicines, including lithium salt and beta blockers, have been reported to trigger or aggravate the disease. Excessive alcohol consumption, smoking and obesity may exacerbate psoriasis or make the management of the condition difficult.[15][16]
Individuals suffering from the advanced effects of the Human immunodeficiency virus, or HIV, often exhibit psoriasis.[17] This presents a paradox to researchers as traditional therapies that reduce T-cell counts generally cause psoriasis to improve. Yet, as CD4-T-cell counts decrease with the progression of HIV, psoriasis worsens.[18] In addition, HIV is typically characterized by a strong Th2 cytokine profile, whereas psoriasis vulgaris is characterized by a strong Th1 secretion pattern.[19] It's hypothesized that the diminished CD4-T-Cell presence causes an over-activation of CD8-T-Cells, which are responsible for the exacerbation of psoriasis in HIV positive patients. It is important to remember that most individuals with psoriasis are otherwise healthy and the presence of HIV accounts for less than 1% of cases. The prevalence of psoriasis in the HIV positive population ranges from 1 to 6 percent, which is about 3 times higher than the normal population.[20]
Psoriasis occurs more likely in dry skin than oily or well-moisturized skin, and specifically after an external skin injury such as a scratch or cut. This is believed to be caused by an infection, in which the infecting organism thrives under dry skin conditions with minimal skin oil, which otherwise protects skin from infections. The case for psoriasis is opposite to the case of athlete's foot, which occurs because of a fungus infection under wet conditions as opposed to dry in psoriasis. This infection induces inflammation, which causes the symptoms commonly associated with psoriasis, such as itching and rapid skin turnover, and leads to drier skin as the infecting organism absorbs the moisture that would otherwise go to the skin. To prevent dry skin and reduce psoriasis symptoms, it is advised to not use shower scrubs, as they not only damage skin by leaving tiny scratches, they also scrape off the naturally occurring skin oil. Additionally, moisturizers can be applied to moisturize the skin, and lotions used to promote skin oil gland functions.[citation needed]
[edit] Treatment
There can be substantial variation between individuals in the effectiveness of specific psoriasis treatments. Because of this, dermatologists often use a trial-and-error approach to finding the most appropriate treatment for their patient. The decision to employ a particular treatment is based on the type of psoriasis, its location, extent and severity. The patient’s age, sex, quality of life, comorbidities, and attitude toward risks associated with the treatment are also taken into consideration.
In 2008, the FDA approved three new treatment options[21] available to psoriasis patients: 1) Taclonex Scalp, a new topical ointment for treating scalp psoriasis; 2) the Xtrac Velocity excimer laser system, which emits a high-intensity beam of ultraviolet light, can treat moderate to severe psoriasis; and 3) the biologic drug adalimumab (brand name Humira) was also approved to treat moderate to severe psoriasis. Adalimumab had already been approved to treat psoriatic arthritis.
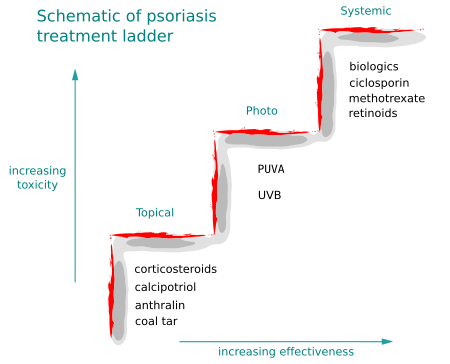
Medications with the least potential for adverse reactions are preferentially employed. If the treatment goal is not achieved then therapies with greater potential toxicity may be used. Medications with significant toxicity are reserved for severe unresponsive psoriasis. This is called the psoriasis treatment ladder.[22] As a first step, medicated ointments or creams, called topical treatments, are applied to the skin. If topical treatment fails to achieve the desired goal then the next step would be to expose the skin to ultraviolet (UV) radiation. This type of treatment is called phototherapy. The third step involves the use of medications which are taken internally by pill or injection. This approach is called systemic treatment.
Over time, psoriasis can become resistant to a specific therapy. Treatments may be periodically changed to prevent resistance developing (tachyphylaxis) and to reduce the chance of adverse reactions occurring. This is called treatment rotation.
Antibiotics are generally not indicated in routine treatment of psoriasis. However, antibiotics may be employed when an infection, such as that caused by the bacteria Streptococcus, triggers an outbreak of psoriasis, as in certain cases of guttate psoriasis.[citation needed]
A psychological symptom management programme has been reported as being a helpful adjunct to traditional therapies in the management of psoriasis.[23]
[edit] Topical treatment
Bath solutions and moisturizers help soothe affected skin and reduce the dryness which accompanies the build-up of skin on psoriatic plaques. Medicated creams and ointments applied directly to psoriatic plaques can help reduce inflammation, remove built-up scale, reduce skin turn over, and clear affected skin of plaques. Ointment and creams containing coal tar, dithranol (anthralin), corticosteroids like desoximetasone (Topicort), vitamin D3 analogues (for example, calcipotriol), and retinoids are routinely used. Argan oil has also been used with some promising results.[24] The mechanism of action of each is probably different but they all help to normalise skin cell production and reduce inflammation. Activated vitamin D and its analogues are highly effective inhibitors of skin cell proliferation.
The disadvantages of topical agents are variably that they can often irritate normal skin, can be time consuming and awkward to apply, cannot be used for long periods, can stain clothing or have a strong odour. As a result, it is sometimes difficult for people to maintain the regular application of these medications. Abrupt withdrawal of some topical agents, particularly corticosteroids, can cause an aggressive recurrence of the condition. This is known as a rebound of the condition.
Some topical agents are used in conjunction with other therapies, especially phototherapy.
[edit] Phototherapy
It has long been recognized that daily, short, non-burning exposure to sunlight helped to clear or improve psoriasis. Niels Finsen was the first physician to investigate the therapeutic effects of sunlight scientifically and to use sunlight in clinical practice. This became known as phototherapy.
Sunlight contains many different wavelengths of light. It was during the early part of the 20th century that it was recognised that for psoriasis the therapeutic property of sunlight was due to the wavelengths classified as ultraviolet (UV) light.
Ultraviolet wavelengths are subdivided into UVA (380–315 nm) UVB (315–280 nm), and UVC (< 280 nm). Ultraviolet B (UVB) (315–280 nm) is absorbed by the epidermis and has a beneficial effect on psoriasis. There are two types of UVB lamps: Narrowband UVB (311 to 312 nm), and Wideband UVB (290-320 nm). UVB Wideband is more effective and it requires shorter exposure time, while UVB Narrowband does not include the spectrum of less than 300 nanometer, and thus considered safer. Exposure to UVB several times per week, over several weeks can help people attain a remission from psoriasis. Sometimes it is needed to continue the treatments once a week as maintenance, or the chronic disease will return.
In Hospitals ultraviolet light treatment is frequently combined with topical (coal tar, calcipotriol) or systemic treatment (retinoids) as there is a synergy in their combination. The Ingram regime, involves UVB and the application of anthralin paste. The Goeckerman regime combines coal tar ointment with UVB. Due to the fact that coal tar includes unknown ingredients, that might cause cancer, the use of coal tar was stopped.
[edit] Photochemotherapy
Psoralen and ultraviolet A phototherapy (PUVA) combines the oral or topical administration of psoralen with exposure to ultraviolet A (UVA) light. Precisely how PUVA works is not known. The mechanism of action probably involves activation of psoralen by UVA light which inhibits the abnormally rapid production of the cells in psoriatic skin. There are multiple mechanisms of action associated with PUVA, including effects on the skin immune system.
PUVA is associated with nausea, headache, fatigue, burning, and itching. Long-term treatment is associated with squamous cell carcinoma (not with melanoma).
[edit] Systemic treatment
Psoriasis which is resistant to topical treatment and phototherapy is treated by medications that are taken internally by pill or injection. This is called systemic treatment. Patients undergoing systemic treatment are required to have regular blood and liver function tests because of the toxicity of the medication. Pregnancy must be avoided for the majority of these treatments. Most people experience a recurrence of psoriasis after systemic treatment is discontinued.
The three main traditional systemic treatments are methotrexate, cyclosporine and retinoids. Methotrexate and cyclosporine are immunosupressant drugs; retinoids are synthetic forms of vitamin A.
Other additional drugs, not specifically licensed for psoriasis, have been found to be effective. These include the antimetabolite tioguanine, the cytotoxic agent hydroxyurea, sulfasalazine, the immunosupressants mycophenolate mofetil, azathioprine and oral tacrolimus. These have all been used effectively to treat psoriasis when other treatments have failed. Although not licensed in many other countries fumaric acid esters have also been used to treat severe psoriasis in Germany for over 20 years.
Biologics are manufactured proteins that interrupt the immune process involved in psoriasis. Unlike generalised immunosuppressant therapies such as methotrexate, biologics focus on specific aspects of the immune function leading to psoriasis. These drugs (interleukin antagonists) are relatively new, and their long-term impact on immune function is unknown. They are very expensive and only suitable for very few patients with psoriasis. Ustekinumab (IL-12 and IL-23 blocker) shows hopeful results for psoriasis therapy.
[edit] Alternative therapy
Climatotherapy involves the notion that some diseases can be successfully treated by living in a particular climate. Several psoriasis clinics are located throughout the world based on this idea. The Dead Sea is one of the most popular locations for this type of treatment.
In Turkey, Croatia (Altermedica) & Ireland, doctor fish which live in the outdoor pools of spas, are encouraged to feed on the psoriatic skin of people with psoriasis. The fish only consume the affected areas of the skin. The outdoor location of the spa may also have a beneficial effect. This treatment can provide temporary relief of symptoms. A revisit to the spas every few months is often required. Treatment in this hot spring has been examined in two small clinical trials, with positive results.[25][26]
[edit] Historical treatment
The history of psoriasis is littered with treatments of dubious effectiveness and high toxicity. These treatments received brief popularity at particular time periods or within certain geographical regions. The application of cat faeces to red lesions on the skin, for example, was one of the earliest topical treatments employed in ancient Egypt. Onions, sea salt and urine, goose oil and semen, wasp droppings in sycamore milk, and soup made from vipers have all been reported as being ancient treatments.
In the more recent past Fowler's solution, which contains a poisonous and carcinogenic arsenic compound, was used by dermatologists as a treatment for psoriasis during the 18th and 19th centuries. Grenz rays (also called ultrasoft X-rays or Bucky rays) was a popular treatment of psoriasis during the middle of the 20th century. This type of therapy was superseded by ultraviolet therapy.
Undecylenic acid was investigated and used for psoriasis some 40 years ago(cir. 1950~).[27]
All these treatments have fallen out of favour.
Sulphur was fashionable as a treatment for psoriasis in the Victorian and Edwardian eras. It has recently re-gained some credibility as a safe alternative to steroids and coal tar.
[edit] Future drug development
Historically, agents used to treat psoriasis were discovered by experimentation or by accident. In contrast, current novel therapeutic agents are designed from a better understanding of the immune processes involved in psoriasis and by the specific targeting of molecular mediators. Examples can be seen in the use of biologics which target T cells and TNF inhibitors.
It has been suggested that cannabis might treat psoriasis, due to the anti-inflammatory properties of its cannabinoids, and the regulatory effects of THC on the immune system.[28] The adverse effects of cannabis might be overcome by use of more specific cannabinoid receptor medications,[29] to inhibit keratinocyte proliferation.[30]
Future innovation should see the creation of additional drugs that refine the targeting of immune-mediators further.[31]
Research into antisense oligonucleotides carries the potential to provide novel therapeutic strategies for treating psoriasis.[32]
ABT-874 is a human anti-IL-12 monoclonal antibody being developed by Abbott Laboratories in conjunction with Cambridge Antibody Technology for the treatment of multiple autoimmune diseases including psoriasis. Phase II trials have been completed and showed promising results.[33] Abbott was planning to initiate Phase III trials in 2007.[34]
In 2004, Tas and Avci [35] demonstrated cyclopamine’s clinical potential for the treatment of psoriasis and basal cell carcinoma in two preliminary proof of concept studies. By treating 31 psoriatic lesions in 7 patients, these authors asserted that topical cyclopamine was more effective in the clinical and histological clearance of guttate and plaque psoriasis than the topical steroid clobetasol-17 propionate.Furthermore, they demonstrated that concurrent application of cylopamine and clobetasol-17 propionate accelerated regression and clearance of selected lesions greater than cyclopamine alone with clearance times as early as 48 hours.They assert that cyclopamine inhibits the abnormal proliferation of epithelial cells, induces terminal differentiation, and is associated with the decreased presence of inflammatory cells, including CD41 lymphocytes.
On August 27, 2006, scientists led by Jeung-Hoon Lee created in the laboratory synthetic lipids called pseudoceramides which are involved in skin cell growth and could be used in treating skin diseases such as atopic dermatitis, a form of eczema characterized by red, flaky and very itchy skin; psoriasis, and glucocorticoid-induced epidermal atrophy, in which the skin shrinks due to skin cell loss.[36]
On November 17, 2008, scientists led by Yin-Ku Lin of Chang Gung Memorial Hospital and Chang Gung University in Taoyuan, Taiwan, told Reuters by telephone that Indigo naturalis (Qing Dai, 青黛), a dark blue plant used in traditional Chinese medicine, appears to be effective in treating psoriasis. In the latest issue of Archives of Dermatology, they wrote, "The indigo naturalis ointment-treated lesions showed an 81 percent improvement, the (non-medicated) ointment-treated lesions showed a 26 percent improvement."[37]
Talarozole amplifies the effects of retinoic acid by inhibiting its metabolism. As of February 2009[update], it is undergoing clinical trials.[38]
[edit] Prognosis
Psoriasis is a lifelong condition.[39] There is currently no cure but various treatments can help to control the symptoms. Many of the most effective agents used to treat severe psoriasis carry an increased risk of significant morbidity including skin cancers, lymphoma and liver disease. However, the majority of people's experience of psoriasis is that of minor localized patches, particularly on the elbows and knees, which can be treated with topical medication. Psoriasis can get worse over time but it is not possible to predict who will go on to develop extensive psoriasis or those in whom the disease may appear to vanish. Individuals will often experience flares and remissions throughout their lives. Controlling the signs and symptoms typically requires lifelong therapy.
According to one study,[40] psoriasis is linked to 2.5-fold increased risk for non melanoma skin cancer in men and women, with no preponderance of any specific histologic subtype of cancer. This increased risk could also be attributed to antipsoriatic treatment.

[edit] "The heartbreak of psoriasis"
The phrase "the heartbreak of psoriasis" is often used both seriously and ironically to describe the emotional impact of the disease. It may include both the effect of having a chronic uncomfortable disorder and the social effects of being self conscious of one's appearance. The term can be found in various advertisements for topical and other treatments; conversely, it has been used to mock the tendency of advertisers to exaggerate (or even fabricate) aspects of a malady for financial gain. While many products today use the phrase in their advertising, it originated in a 1960s advertising campaign for Tegrin, a coal tar-based ointment.
[edit] See also
[edit] References
- ^ http://www.emedicine.com/derm/topic365.htm#section~clinical see causes
- ^ Shai A, Vardy D, Zvulunov A (2002). "[Psoriasis, biblical afflictions and patients' dignity]" (in Hebrew). Harefuah 141 (5): 479–82, 496. PMID 12073533.
- ^ Glickman FS (1986). "Lepra, psora, psoriasis". J. Am. Acad. Dermatol. 14 (5 Pt 1): 863–6. doi:. PMID 3519699.
- ^ "Application to dermatology of International Classification of Disease (ICD-10) - ICD sorted by code: L40.000 - L41.000", The International League of Dermatological Societies
- ^ "Erythrodermic psoriasis", New Zealand Dermatological Society
- ^ Freedberg, et. al. (2003). Fitzpatrick's Dermatology in General Medicine. (6th ed.). McGraw-Hill. ISBN 0071380760.
- ^ James, William; Berger, Timothy; Elston, Dirk (2005). Andrews' Diseases of the Skin: Clinical Dermatology. (10th ed.). Saunders. ISBN 0721629210.
- ^ "Psoriasis Update -Skin & Aging". http://www.skinandaging.com/article/5394. Retrieved on 2007-07-28.
- ^ Louden BA, Pearce DJ, Lang W, Feldman SR (2004). "A Simplified Psoriasis Area Severity Index (SPASI) for rating psoriasis severity in clinic patients". Dermatol. Online J. 10 (2): 7. PMID 15530297.
- ^ "Coping With Psoriasis" Parade.com
- ^ Gelfand JM et al (2005). "Prevalence and Treatment of Psoriasis in the United Kingdom". Arch. Dermatol. 141 (12): 1537–1541. doi:. PMID 16365254.
- ^ "BENCHMARK SURVEY ON PSORIASIS AND PSORIATIC ARTHRITIS: SUMMARY OF TOP-LINE RESULTS" (PDF). NATIONAL PSORIASIS FOUNDATION. http://www.psoriasis.org/files/pdfs/press/npfsurvey.pdf.
- ^ Krueger G, Ellis CN (2005). "Psoriasis--recent advances in understanding its pathogenesis and treatment". J. Am. Acad. Dermatol. 53 (1 Suppl 1): S94–100. doi:. PMID 15968269.
- ^ Zenz R, Eferl R, Kenner L, et al (2005). "Psoriasis-like skin disease and arthritis caused by inducible epidermal deletion of Jun proteins". Nature 437 (7057): 369–75. doi:. PMID 16163348.
- ^ [1] Psoriasis Triggers at Psoriasis Net. SkinCarePhysicians.com 9-28-05. American Academy of Dermatology, 2008.
- ^ Behnam SM, Behnam SE, Koo JY (2005). "Smoking and psoriasis". Skinmed 4 (3): 174–6. doi:. PMID 15891254. http://www.lejacq.com/articleDetail.cfm?pid=SKINmed_4;3:174.
- ^ [2][3] Fife, Jeffes, Koo, Waller. Unraveling the Paradoxes of HIV-associated Psoriasis: A Review of T-cell Subsets and Cytokine Profiles. 5-18-07. Retrieved 5-13-08.
- ^ Ortonne JP, Lebwohl M, Em Griffiths C (2003). "Alefacept-induced decreases in circulating blood lymphocyte counts correlate with clinical response in patients with chronic plaque psoriasis". Eur J Dermatol 13 (2): 117–23. PMID 12695125. http://www.john-libbey-eurotext.fr/medline.md?issn=1167-1122&vol=13&iss=2&page=117.
- ^ Austin LM, Ozawa M, Kikuchi T, Walters IB, Krueger JG (November 1999). "The majority of epidermal T cells in Psoriasis vulgaris lesions can produce type 1 cytokines, interferon-gamma, interleukin-2, and tumor necrosis factor-alpha, defining TC1 (cytotoxic T lymphocyte) and TH1 effector populations: a type 1 differentiation bias is also measured in circulating blood T cells in psoriatic patients". J. Invest. Dermatol. 113 (5): 752–9. doi:. PMID 10571730.
- ^ [4] A Case Report of Severe Psoriasis in a Patient with AIDS: The Role of the HIV Virus and the Therapeutic Challenges Involved. Vol: 13 No 2, 2002. National Skin Center. Retrieved 05-13-08.
- ^ "Psoriasis Medical Breakthroughs" Parade.com
- ^ Lofholm PW (2000). "The psoriasis treatment ladder: a clinical overview for pharmacists". US Pharm 25 (5): 26–47. http://www.uspharmacist.com/oldformat.asp?url=newlook/files/Feat/apr00pro.cfm&pub_id=8&article_id=511.
- ^ "Research Findings Register: summary number 637". http://www.refer.nhs.uk/ViewRecord.asp?ID=637&Print=1. Retrieved on 2007-07-22.
- ^ "Irishman hits on 'cure' for psoriasis". Belfast Telegraph. December 12, 2007. http://www.belfasttelegraph.co.uk/news/local-national/article3247531.ece. Retrieved on 2007-12-13.
- ^ Ozçelik S, Polat HH, Akyol M, Yalçin AN, Ozçelik D, Marufihah M (June 2000). "Kangal hot spring with fish and psoriasis treatment". J. Dermatol. 27 (6): 386–90. PMID 10920584.
- ^ Grassberger M, Hoch W (December 2006). "Ichthyotherapy as alternative treatment for patients with psoriasis: a pilot study". Evid Based Complement Alternat Med 3 (4): 483–8. doi:. PMID 17173112.
- ^ Ereaux L, Craig G (October 1949). "The Oral Administration Of Undecylenic Acid In The Treatment Of Psoriasis" (PDF). Canad. M. A. J. 61: 361–4. http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1591667&blobtype=pdf. Retrieved on 2007-01-05. - see page 4/364 of link
- ^ Namazi MR (2005). "Cannabinoids, loratadine and allopurinol as novel additions to the antipsoriatic ammunition". Journal of the European Academy of Dermatology and Venereology : JEADV 19 (3): 319–22. doi:. PMID 15857457.
- ^ Fowler CJ (2005). "Pharmacological properties and therapeutic possibilities for drugs acting upon endocannabinoid receptors". Current drug targets. CNS and neurological disorders 4 (6): 685–96. doi:. PMID 16375686.
- ^ Wilkinson JD, Williamson EM (2007). "Cannabinoids inhibit human keratinocyte proliferation through a non-CB1/CB2 mechanism and have a potential therapeutic value in the treatment of psoriasis". J. Dermatol. Sci. 45 (2): 87–92. doi:. PMID 17157480.
- ^ Nickoloff BJ, Nestle FO (2004). "Recent insights into the immunopathogenesis of psoriasis provide new therapeutic opportunities". J. Clin. Invest. 113 (12): 1664–75. doi:. PMID 15199399.
- ^ White PJ, Atley LM, Wraight CJ (2004). "Antisense oligonucleotide treatments for psoriasis". Expert opinion on biological therapy 4 (1): 75–81. doi:. PMID 14680470.
- ^ Heller M. (2007) Positive results for ABT-874 in the treatment of psoriasis J Drugs Dermatol
- ^ Cambridge Antibody Technology | ABT-874
- ^ [Tas S, Avci O. Rapid clearance of psoriatic skin lesions induced by topical cyclopamine. Dermatology 2004;209:126-31]
- ^ Science Daily, New Skin-healing Chemicals
- ^ Indigo plant may treat chronic skin disease (Reuters)
- ^ Giltaire, S; Herphelin F, Frankart A, Hérin M, Stoppie P, Poumay Y (11 December 2008). "The CYP26 inhibitor R115866 potentiates the effects of all-trans retinoic acid on cultured human epidermal keratinocytes". Br J Dermatol. PMID 19120344.
- ^ Jobling R (2007). "A patient's journey:Psoriasis". Br Med J 334: 953–4. doi:. PMID 17478850.
- ^ Olsen JH, Frentz G, Møller H (1993). "[Psoriasis and cancer]" (in Danish). Ugeskr. Laeg. 155 (35): 2687–91. PMID 8212383.
[edit] External links
| Wikimedia Commons has media related to: Psoriasis |
[edit] Research and non-commercial
- "Questions and Answers about Psoriasis" at National Institute of Arthritis and Musculoskeletal and Skin Diseases
- Psoriasis at National Institute of Arthritis and Musculoskeletal and Skin Diseases
- Psoriasis at Mayo Clinic
- The Psoriasis Association
- National Psoriasis Foundation Homepage
- Psoriasis Cure Now Homepage
- Psoriasis Support Canada
- Psoriasis Help Homepage
- DermAtlas 7
- Psoriasis in Literature
- The Psoriasis and Psoriatic Arthritis Alliance (PAPAA) - UK national charity
- - International Association of Psoriasis Associations - IFPA
[edit] Books
- From Arsenic to Biologicals: A 200 Year History of Psoriasis (Barbara S. Baker), ISBN 0-955-16032-4.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||

