Bupropion
From Wikipedia, the free encyclopedia
 |
|
 |
|
|
Bupropion
|
|
| Systematic (IUPAC) name | |
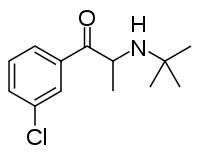
| (±)-2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one | |
| Identifiers | |
| CAS number | |
| ATC code | N06 |
| PubChem | |
| DrugBank | |
| ChemSpider | |
| Chemical data | |
| Formula | C13H18ClNO |
| Mol. mass | 239.74 g/mol |
| SMILES | & |
| Pharmacokinetic data | |
| Bioavailability | 5 to 20% in animals; no studies in humans |
| Metabolism | Hepatic—important CYP2B6 and 2D6 involvement |
| Half life | 20 hours |
| Excretion | Renal (87%), fecal (10%) |
| Therapeutic considerations | |
| Pregnancy cat. | |
| Legal status | |
| Routes | Oral |
Bupropion (INN, previously known as amfebutamone;[1] Wellbutrin, Zyban) is an atypical antidepressant that acts as a norepinephrine and dopamine reuptake inhibitor, and nicotinic antagonist.[2][3] Bupropion belongs to the chemical class of aminoketones and is similar in structure to the stimulant cathinone, to the anorectic diethylpropion, and to phenethylamines in general.
Initially researched and marketed as an antidepressant, bupropion was subsequently found to be effective as a smoking cessation aid. In 2007 it was the fourth-most prescribed antidepressant in the United States retail market, with 20.184 million retail prescriptions.[4]
Bupropion lowers seizure threshold and its potential to cause seizures was widely publicized. However, at the recommended dose the risk of seizures is comparable to that observed for other antidepressants. Bupropion is an effective antidepressant on its own but it is particularly popular as an add-on medication in the cases of incomplete response to the first-line SSRI antidepressant. In contrast to many psychiatric drugs, including nearly all antidepressants, bupropion does not cause weight gain or sexual dysfunction.
Contents |
[edit] History
Bupropion was invented by Nariman Mehta of Burroughs Wellcome (now GlaxoSmithKline) in 1969, and the US patent for it was granted in 1974.[5] It was approved by the United States Food and Drug Administration (FDA) as an antidepressant on December 30, 1985 and marketed under the name Wellbutrin.[6] However, a significant incidence of seizures at the originally recommended dosage (400–600 mg) caused the withdrawal of the drug in 1986. Subsequently, the risk of seizures was found to be highly dose-dependent, and bupropion was re-introduced to the market in 1989 with a maximum recommended dose of 450 mg/day.

In 1996, the FDA approved a sustained-release formulation of bupropion called Wellbutrin SR, intended to be taken twice a day (as compared to three times a day for immediate-release Wellbutrin).[7] In 2003 the FDA approved another sustained-release formulation called Wellbutrin XL, intended for once-daily dosing. Wellbutrin SR and XL are available in generic form in the United States, while in Canada, only the SR formulation is available in generic form. In 1997, bupropion was approved by the FDA for use as a smoking cessation aid under the name Zyban.[7] In 2006, Wellbutrin XL was similarly approved as a treatment for seasonal affective disorder.[8]
[edit] Therapeutic uses
[edit] Depression
Placebo-controlled double-blind clinical studies have confirmed the efficacy of bupropion for clinical depression.[9] Comparative clinical studies demonstrated the equivalency of bupropion and sertraline (Zoloft), fluoxetine (Prozac), paroxetine (Paxil)[10] and escitalopram (Lexapro)[11] as antidepressants. A significantly higher remission rate with bupropion treatment than for venlafaxine (Effexor) was observed in a recent study.[12] Unlike all other antidepressants, except mirtazapine (Remeron), maprotiline (Ludiomil) and tianeptine (Stablon), bupropion does not cause sexual dysfunction and the occurrence of sexual side effects is not different from placebo.[13][14] Bupropion treatment is not associated with weight gain; on the contrary, at the end of every study comparing bupropion with placebo or other antidepressants the bupropion group had a lower average weight.[15] Bupropion is more effective than SSRIs at improving symptoms of hypersomnia and fatigue in depressed patients.[16] In a comparative meta-analysis, there appeared to be a modest advantage for the SSRIs compared to bupropion in the treatment of depression with high anxiety, while these medications were equivalent for the depression with moderate or low anxiety.[17]
According to several surveys, the augmentation of a prescribed SSRI with bupropion is the preferred strategy among clinicians when the patient does not respond to the SSRI.[18] For example, the combination of bupropion and citalopram (Celexa) was observed to be more effective than switching to another antidepressant. The addition of bupropion to an SSRI (primarily fluoxetine or sertraline) resulted in a significant improvement in 70–80% of patients who had an incomplete response to the first-line antidepressant.[19][20] Bupropion improved ratings of "energy", which had decreased under the influence of the SSRI; also noted were improvements of mood and motivation, and some improvement of cognitive and sexual functions. Sleep quality and anxiety ratings in most cases were unchanged.[20] In the STAR*D study, the patients who did not respond to citalopram (Celexa) were randomly assigned to augmentation by bupropion or buspirone (Buspar). Approximately 30% of subjects in both groups achieved a remission. However, bupropion augmentation gave better results based on the patients' self-ratings and was much better tolerated. The authors observed that "these findings reveal a consistently more favorable outcome with sustained-release bupropion than with buspirone augmentation of citalopram."[21] The same study indicated a possibility of higher remission rate when the non-responders to citalopram received bupropion augmentation rather than were switched to bupropion (30% vs. 20%).[22]
[edit] Smoking cessation
Bupropion reduces the severity of nicotine cravings and withdrawal symptoms. After a seven-week treatment, 27% of subjects who received bupropion reported that an urge to smoke was a problem, versus 56% of those who received placebo. In the same study, 21% of the bupropion group reported mood swings, versus 32% of the placebo group.[23] The bupropion treatment course lasts for seven to twelve weeks, with the patient halting the use of tobacco about ten days into the course. The efficacy of bupropion is similar to that of nicotine replacement therapy. Bupropion approximately doubles the chance of quitting smoking successfully after three months. One year after the treatment, the odds of sustaining smoking cessation are still 1.5 times higher in the bupropion group than in the placebo group.[24] The combination of bupropion and nicotine appears not to further increase the cessation rate. In a direct comparison, varenicline (Chantix) showed superior efficacy: after one year, the rate of continuous abstinence was 10% for placebo, 15% for bupropion, and 23% for varenicline.[25] Bupropion slows the weight gain that often occurs in the first weeks after quitting smoking (after seven weeks, the placebo group had an average 2.7 kg increase in weight, versus 1.5 kg for the bupropion group). With time, however, this effect becomes negligible (after 26 weeks, both groups recorded an average 4.8 kg weight gain).[23]
[edit] Sexual dysfunction
According to a survey, bupropion is the drug of choice among psychiatrists for the treatment of SSRI-induced sexual dysfunction, although it is not an FDA-approved indication. Thirty-six percent of responding psychiatrists preferred switching patients with SSRI-induced sexual dysfunction to bupropion; however, 43 percent favored the augmentation of the current medication with bupropion.[26] There are studies demonstrating the efficacy of both approaches; improvement of the desire and orgasm components of sexual function were the most often noted. For the augmentation approach, the addition of at least 200 mg/day of bupropion to the SSRI regimen may be necessary to achieve an improvement since the addition of 150 mg/day of bupropion did not produce a statistically significant difference from placebo.[27][28][29][30][31][32]
Several studies have indicated that bupropion also relieves sexual dysfunction in people who do not have depression. In a mixed-gender double-blind study, 63% of subjects on a 12-week course of bupropion rated their condition as improved or much improved, versus 3% of subjects on placebo.[33] Two studies, one of which was placebo-controlled, demonstrated the efficacy of bupropion for women with hypoactive sexual desire,[34][35] resulting in significant improvement of arousal, orgasm and overall satisfaction. Bupropion also showed promise as a treatment for sexual dysfunction caused by chemotherapy for breast cancer[36] and for orgasmic dysfunction.[37] As with the treatment of SSRI-induced sexual disorder, a higher dose of bupropion (300 mg) may be necessary: a randomized study employing a lower dose (150 mg) failed to find a significant difference between bupropion, sexual therapy or combined treatment.[38] Bupropion does not affect any measures of sexual functioning in healthy men.[39]
[edit] Obesity
A recent meta-analysis of anti-obesity medications pooled the results of three double-blind, placebo-controlled trials of bupropion. It confirmed the efficacy of bupropion given at 400 mg per day for treating obesity. Over a period of 6 to 12 months, weight loss in the bupropion group (4.4 kg) was significantly greater than in the placebo group (1.7 kg). The same review found the differences in weight loss between bupropion and other established weight-loss medications, such as sibutramine, orlistat and diethylpropion, to be statistically insignificant.[40]
[edit] Attention-deficit hyperactivity disorder
Although attention-deficit hyperactivity disorder (ADHD) is not an approved indication, bupropion was found to be effective for adult ADHD.[41] There have been many positive case studies and other uncontrolled clinical studies of bupropion for ADHD in minors.[42] However, in the largest to date double-blind study, which was conducted by GlaxoSmithKline, the results were inconclusive. Aggression and hyperactivity as rated by the children's teachers were significantly improved in comparison to placebo; in contrast, parents and clinicians could not distinguish between the effects of bupropion and placebo.[42] The 2007 guideline on the ADHD treatment from American Academy of Child and Adolescent Psychiatry notes that the evidence for bupropion is "far weaker" than for the FDA-approved treatments. Its effect may also be "considerably less than of the approved agents... Thus it may be prudent for the clinician to recommend a trial of behavior therapy at this point, before moving to these second-line agents."[43] Similarly, the 2006 guideline from the Texas Department of State Health Services recommends considering bupropion or a tricyclic antidepressant as a fourth-line treatment after trying two different stimulants and atomoxetine (Strattera).[44][45]
A study of prophylactic bupropion for the prevention of smoking among teenagers with ADHD yielded unexpected results. The teenagers taking bupropion were two times more likely (close to statistical significance) to begin smoking than the teenagers in the placebo group. At the same time, the sub-group of patients taking stimulants in addition to bupropion or placebo had a five times lower risk of smoking initiation.[46]
[edit] Other uses
Bupropion has been approved by the FDA[47] for the prevention of seasonal affective disorder.[48] There is considerable disagreement regarding whether it is useful to add an antidepressant, including bupropion, to a mood stabilizer in patients with bipolar depression.[49][50][51]
No properly controlled double-blind studies of bupropion for Parkinson's disease have been conducted. A small 1984 study funded by bupropion's manufacturer found that addition of bupropion to carbidopa or levodopa improved Parkinson's symptoms in ten out of twenty patients; however, the side effects, particularly nausea and vomiting, were frequent.[52] The American Psychiatric Association notes that, "there is no evidence favoring any particular antidepressant medication from the standpoint of therapeutic efficacy in patients with Parkinson’s disease complicated by major depressive disorder."[53]
[edit] Contraindications
GlaxoSmithKline advises that bupropion should not be prescribed to individuals with epilepsy or other conditions that lower the seizure threshold, such as alcohol or benzodiazepine discontinuation, anorexia nervosa, bulimia, or active brain tumors. It should be avoided in individuals who are also taking MAO inhibitors (MAOIs). When switching from MAOIs to bupropion, it is important to include a washout period of about two weeks between the medications.[54] The prescribing information approved by the FDA recommends that caution should be exercised when treating patients with liver damage, severe kidney disease, and severe hypertension, as well as in pediatric patients, adolescents and young adults due to the increased risk of suicidal ideation.[54]
According to a retrospective case series published in 1993, bupropion treatment may exacerbate tics in children with co-occurring ADHD and Tourette syndrome.[55] No further research of this side effect has been conducted.
[edit] Risk of suicide
The FDA requires all antidepressants, including bupropion, to carry a black box warning stating that antidepressants may increase the risk of suicide in persons younger than 25. This warning is based on a statistical analysis conducted by the FDA which found a 2-fold increase of the suicidal ideation and behavior in children and adolescents, and 1.5-fold increase of suicidality in the 18–24 age group.[56]
Suicidal ideation and behavior in clinical trials are rare. For the above analysis, the FDA combined the results of 295 trials of 11 antidepressants for psychiatric indications in order to obtain statistically significant results. Considered separately, bupropion and nine other antidepressants were not statistically different from placebo. Only fluoxetine caused a significant decrease in suicidal ideation.[56]
Suicidal behavior is even less likely when bupropion is prescribed for smoking cessation. According to a Cochrane Database review, there have been four suicides per one million prescriptions and one case of suicidal ideation per ten thousand prescriptions of bupropion for smoking cessation in the UK. The review concludes, "Although some suicides and deaths while taking bupropion have been reported, thus far there is insufficient evidence to suggest they were caused by bupropion."[57]
[edit] Adverse effects

The common adverse effects associated with 12-hour sustained-release bupropion (with the greatest difference from placebo) are dry mouth, nausea, insomnia, tremor, excessive sweating and tinnitus. Those that most often resulted in interruption of the treatment in the same trial were rash (2.4%) and nausea (0.8%). The development of mild to moderate skin rashes is associated with sensitivity to dye components within the pill coating. This can often be alleviated simply by prescribing a differently colored pill.[54]
Seizure is the most controversial side effect of bupropion, and was responsible for its initial withdrawal from the market. The risk of seizure is highly dose-dependent: 0.1% at 100–300 mg of bupropion, 0.4% at 300–450 mg, and 2% at 600 mg. For comparison, the incidence of the first unprovoked seizure in the general population is 0.07–0.09%. The risk of seizure for other antidepressants is as follows: 0.1–0.6% for imipramine, depending on dosage; 0–0.06% for amitriptyline, depending on dosage; 0.5% for clomipramine; 0.4% for maprotiline; and 0.2% for fluoxetine and fluvoxamine.[58] Experiments on mice indicate that increased susceptibility to seizure is a general side effect of chronically using antidepressants that inhibit norepinephrine transporter, such as imipramine, desipramine and reboxetine.[59] Clinical depression itself was reported to increase the occurrence of seizures two-to-sevenfold compared with the general population; in this light, the above statistics could indicate that low to moderate doses of antidepressants, including bupropion, may actually have an anti-convulsive action.[60]
There is evidence of several neuropsychiatric symptoms associated with bupropion in patients with depression, including delusions, hallucinations, psychosis, concentration disturbance, paranoia, and confusion. In some cases, these symptoms are reduced or eliminated by decreasing the dose or ceasing treatment. The prescribing information notes that "it is generally believed (though not established in controlled trials)" that, should an episode of depression actually be the first presentation of bipolar disorder, treating it with antidepressants, including bupropion, may precipitate a manic episode.[54] More recent data indicate that the addition of newer antidepressants, including bupropion, to a mood stabilizer does not cause the switch to mania more often than the addition of placebo.[50] Moreover, when added to a mood stabilizer, bupropion and sertraline had a twice lower switch risk than venlafaxine.[61]
The prescribing information notes that hypertension, sometimes severe, was observed in some patients, both with and without pre-existing hypertension. The frequency of this adverse effect was under 1% and not significantly higher than that found with placebo.[54] In a group of cardiac patients with depression, high doses of bupropion (400–500 mg/day) caused a rise in supine blood pressure but had no effect on pulse rate.[62] No statistically significant changes in blood pressure or heart rate occurred in patients with or without heart conditions at a lower dose of 300 mg/day.[63] In a study of bupropion for ADHD, a rise of systolic blood pressure by 6 mm Hg and of heart rate by 7 beats per minute (both statistically significant) were observed.[64] A study of smokers hospitalized for heart disease found a 1.5-fold increase (close to being statistically significant) in subsequent cardiovascular events in the bupropion group, compared with the placebo group, but found no difference in blood pressure.[65] Although the cardiovascular side effects of bupropion appear to be mild, it cannot be recommended for patients with heart disease, since the safety comparison with SSRIs (such as sertraline and fluoxetine, which may have a preventative effect after a myocardial infarction[66]) is not in its favor.
In the UK, more than 7,600 reports of suspected adverse reactions were collected in the first two years after bupropion's approval by the MHRA as part of the Yellow Card Scheme, which monitored side effects. Approximately 540,000 people were treated with bupropion for smoking cessation during that period. The MHRA received 60 reports of "suspected [emphasis MHRA's] adverse reactions to Zyban which had a fatal outcome". The agency concluded that "in the majority of cases the individual’s underlying condition may provide an alternative explanation."[67] This is consistent with a large, 9,300-patient safety study that showed that the mortality of smokers taking bupropion is not higher than the natural mortality of smokers of the same age.[68]
According to several case reports, stopping bupropion abruptly may result in discontinuation syndrome expressed as dystonia, irritability, anxiety, mania, headache, aches and pains.[69][70][71][72]
Other isolated adverse affects have been reported. Three cases of liver toxicity have been described in the literature,[73] a very low incidence given the widespread use of the drug. A single case of clitoral priapism (clitorism) has been reported in the literature.[74]
[edit] Overdose
Overdose of bupropion results in significant clinical effects in over one-third of cases.[75] The most common symptoms include sinus tachycardia, hypertension, drowsiness, lethargy, agitation, nausea and vomiting, and in particular delirium and seizures.[75][76][77] Less commonly additional symptoms include auditory and visual hallucinations,[78] coma,[77] and ECG changes such as conduction disturbance or arrhythmia.[79][80][81]
In the majority of childhood exploratory ingestions involving one or two tablets, children will remain asymptomatic.[82][83] In teenagers and adults seizures are more commonly observed with the seizure rate increasing tenfold with doses of 600 mg daily.[84] One overdose study suggested a dose-dependent relationship with seizures; patients ingesting more than 4.5 g were likely to have a seizure and nearly all patients ingesting more than 9 g had a seizure.[75]
There is no specific antidote for bupropion; treatment is supportive, and focuses on maintaining airway patency and controlling seizures with high dose intravenous benzodiazepines or barbiturates if seizures are refractory to benzodiazepines.[76] Gastric decontamination may be of little benefit given the risk of seizures and aspiration[76] but activated charcoal is recommended,[75] additionally whole bowel irrigation should be undertaken in those ingesting sustained release formulations.[76] Toxic effects may be delayed in onset, with seizures developing as late as 32 hours,[76] subsequently patients should undergo electroencephalographic monitoring for 48 hours.[54]
Bupropion overdose rarely results in death, although cases have been reported.[79][85][86] Fatalities are typically associated with large overdosage and related to metabolic acidosis and hypoxia as complications of status epilepticus with associated cardiorespiratory arrest.[87] There is one published case report of successful treatment of refractory cardiac arrest in overdose of bupropion and lamotrigine using lipid rescue.[88]
[edit] Mechanism of action
Bupropion is a dopamine and norepinephrine reuptake inhibitor.[89] It is about twice as potent an inhibitor of dopamine reuptake than of norepinephrine reuptake. As bupropion is rapidly converted in the body into several metabolites with differing activity, its action cannot be understood without reference to its metabolism. The occupancy of dopamine transporter (DAT) by bupropion and its metabolites in the human brain as measured by positron emission tomography was 6–22% in an independent study[90] and 12–35% according to GlaxoSmithKline researchers.[91] Based on analogy with serotonin reuptake inhibitors, higher than 50% inhibition of DAT would be needed for the dopamine reuptake mechanism to be a major mechanism of the drug's action. Bupropion does not inhibit monoamine oxidase or serotonin reuptake. However, it has been shown to indirectly enhance the firing of serotonergic neurons, via activation of downstream norepinephrine flow. Bupropion has also been shown to act as a noncompetitive α3β4 nicotinic antagonist.[92] The degree of inhibition of α3β4 receptors correlates well with the decrease in self-administration of morphine and methamphetamine in rats,[93] and may be relevant to the effect of bupropion on nicotine addiction. The drug is supplied as a racemic mixture, and no studies have been published on the activities of the individual enantiomers.[94]
[edit] Pharmacokinetics

Bupropion is metabolized in the liver. It has several active metabolites: R,R-hydroxybupropion, S,S-hydroxybupropion, threo-hydrobupropion and erythro-hydrobupropion, which are further metabolized to inactive metabolites and eliminated through excretion into the urine. Pharmacological data on bupropion and its metabolites are presented in Table 1. Bupropion is known to weakly inhibit the α1 adrenaline receptor, with a 14% potency of its dopamine uptake inhibition, and the H1 receptor, with a 9% potency.[95]
The biological activity of bupropion can be attributed to a significant degree to its active metabolites, in particular to S,S-hydroxybupropion. GlaxoSmithKline developed this metabolite as a separate drug called radafaxine,[96] but discontinued development in 2006 due to "an unfavourable risk/benefit assessment".[97]
Bupropion is metabolized to hydroxybupropion by CYP2B6, an isoenzyme of the cytochrome P450 system. Alcohol causes an increase of CYP2B6 in the liver, and persons with a history of alcohol use metabolize bupropion faster. The mechanism of formation of erythro-hydrobupropion and threo-hydrobupropion has not been studied but is probably mediated by one of the carbonyl reductase enzymes. The metabolism of bupropion is highly variable: the effective doses of bupropion received by persons who ingest the same amount of the drug may differ by as much as 5.5 times (and the half-life from 3 to 16 hours), and of hydroxybupropion by as much as 7.5 times (and the half-life from 12 to 38 hours).[98][99] Based on this, some researchers have advocated monitoring of the blood level of bupropion and hydroxybupropion.[100]
There are significant interspecies differences in the metabolism of bupropion, with guinea pigs' metabolism of the drug being closest to that of humans.[101] Particular caution is needed when extrapolating the results of experiments on rats to humans since hydroxybupropion, the main metabolite of bupropion in humans, is absent in rats.[102]
There have been two reported cases of false-positive urine amphetamine tests in persons taking bupropion. Bupropion metabolites erythro-hydrobupropion and threo-hydrobupropion, which have a phenethylamine structure resembling amphetamine are likely to have been responsible for this reaction. More specific follow-up tests were negative.[103][104]
| Exposure (concentration over time; bupropion exposure = 100%) and half-life | |||||
| Bupropion | R,R- Hydroxy bupropion |
S,S- Hydroxy bupropion |
Threo- hydro bupropion |
Erythro- hydro bupropion |
|
|---|---|---|---|---|---|
| Exposure | 100% | 800% | 160% | 310% | 90% |
| Half-life | 10 h (IR) 17 h (SR) |
21 h | 25 h | 26 h | 26 h |
| Inhibition potency (potency of DA uptake inhibition by bupropion = 100%) | |||||
| DA uptake | 100% | 0% (rat) | 70% (rat) | 4% (rat) | No data |
| NE uptake | 27% | 0% (rat) | 106% (rat) | 16% (rat) | No data |
| Ser uptake | 2% | 0% (rat) | 4%(rat) | 3% (rat) | No data |
| α3β4 nicotinic | 53% | 15% | 10% | 7% (rat) | No data |
| α4β2 nicotinic | 8% | 3% | 29% | No data | No data |
| α1* nicotinic | 12% | 13% | 13% | No data | No data |
| DA = dopamine; NE = norepinephrine; Ser = serotonin. | |||||
[edit] Interactions
Since bupropion is metabolized to hydroxybupropion by the CYP2B6 enzyme, drug interactions with CYP2B6 inhibitors are possible: this includes medications like paroxetine, sertraline, norfluoxetine (the active metabolite of fluoxetine), diazepam, clopidogrel, and orphenadrine. The expected result is the increase of bupropion and decrease of hydroxybupropion blood concentration. The reverse effect (decrease of bupropion and increase of hydroxybupropion) can be expected with CYP2B6 inducers, such as carbamazepine, clotrimazole, rifampicin, ritonavir, St John's Wort and others.[109]
Hydroxybupropion (but not bupropion) is itself an inhibitor of CYP2D6, as well as a substrate of that enzyme. A significant increase in the concentration of some drugs metabolized by CYP2D6 (venlafaxine, desipramine and dextromethorphan, but not fluoxetine or paroxetine) has been observed when they are taken with bupropion.[109][110] It is also important to note that prodrugs such as Codeine may not be effective when combined with Bupropion due to Hydroxybupropion's inhibition of CYP2D6.
Bupropion lowers the seizure threshold; accordingly, extreme care should be taken when prescribing bupropion with other medications that also lower it, such as antipsychotics, theophylline, steroids, and some tricyclic antidepressants.[54] Its combination with nicotine replacement therapies can elevate blood pressure; since this combination is no more effective than either a nicotine patch or bupropion alone, it is not recommended.
The prescribing information recommends minimizing the use of alcohol, since in rare cases bupropion reduces alcohol tolerance, and because the excessive use of alcohol may lower the seizure threshold.[54] A small study conducted by GlaxoSmithKline indicated that bupropion (100 mg) may counteract the subjective effects of small doses of alcohol (16–32 mL, slightly less than 1–2 standard US drinks). The volunteers reported feeling more sober and clear-headed and less sedated. Bupropion also reduced the detrimental effect of alcohol on auditory vigilance. The combination of bupropion (100 mg) and two drinks of alcohol increased heart rate by six beats per minute, a statistically significant increase.[111]
[edit] Availability and dose forms

Brand-name and generic bupropion tablets are available in three forms, each as the hydrochloride salt: immediate release (Wellbutrin), sustained release (Wellbutrin SR), and extended release (Wellbutrin XL or XR). "Sustained release" and "extended release" are generally interchangeable terms, but in this case Wellbutrin SR is intended for twice-daily dosing and Wellbutrin XL is intended for once-daily dosing. Not all generics have retained this naming scheme, and the United States Pharmacopeia requires all prolonged-release drug formulations (including generics for Wellbutrin SR) to be labeled "extended release", which has caused confusion and medication errors.[112][113] According to GlaxoSmithKline, a 150 mg Wellbutrin SR tablet can be split in two and retain its sustained-release characteristics.[114] An extended-release form of bupropion hydrobromide was approved by the FDA in April 2008. It will be marketed under the trade name Aplenzin.[115]
On October 11, 2007, two providers of consumer information on nutritional products and supplements, ConsumerLab.com and The People’s Pharmacy, released the results of comparative tests of different brands of bupropion.[116] The People's Pharmacy received multiple reports of increased side effects and decreased efficacy of generic bupropion, which prompted it to ask ConsumerLab.com to test the products in question. The tests showed that "one of a few generic versions of Wellbutrin XL 300 mg, sold as Budeprion XL 300 mg, didn't perform the same as the brand-name pill in the lab."[117] The FDA investigated these complaints and concluded that the Budeprion XL is equivalent to Wellbutrin XL in regard to bioavailability of bupropion and its main active metabolite hydroxybupropion. The FDA also noted that the coincidental natural mood variation is the most likely explanation for the apparent worsening of depression after the switch from Wellbutrin XL to Budeprion XL.[118]
In France, marketing authorization was granted on August 3, 2001, also solely as a smoking cessation aid, and with a maximum daily dose of 300 mg;[119] only sustained-release bupropion is available. Bupropion was granted a licence for use in adults with major depression in the Netherlands in early 2007, with GlaxoSmithKline expecting subsequent approval in other European countries.[120]
[edit] Abuse liability
According to the US government classification of psychiatric medications, bupropion is "non-abusable"[121] or has low abuse potential.[122] In animal studies, however, squirrel monkeys[123] and rats[124] maintained the intravenous self-administration of bupropion, which may indicate abuse potential. However, significant interspecies differences of bupropion metabolism, particularly between rats and humans, make such extrapolations questionable.[102]
Two studies on drug abusers indicated that the subjective effects of bupropion are markedly different from those of amphetamine.[125][126] Healthy volunteers trained to discriminate amphetamine and placebo recognized bupropion (400 mg) as amphetamine 20% of the time, compared to 10% for placebo and 75% for methylphenidate (20 mg). They also reported feeling alert, vigorous, elated and energetic, reflecting the general stimulating properties of bupropion. In contrast to amphetamine and methylphenidate, there was no feeling of "liking the drug" and no desire to take it again.[127] A comparison of bupropion SR (150 mg) and caffeine (178 mg) indicated that caffeine may have higher abuse liability since it resulted in more reports of pleasant feelings and a "high" than bupropion.[128]
There have been four reports of bupropion abuse in the literature. Three cases described teenagers crushing and insufflating (snorting) the drug, two of them resulting in seizures.[129][130][131] An additional case was reported where a teenager ingested bupropion believing the drug to be a stimulant.[132] An article on medication abuse in prisons mentions bupropion as one of the psychotropic medications commonly abused by inmates.[133]
[edit] Synthesis
Bupropion is synthesized by brominating 3'-chloropropiophenone, followed by nucleophilic substitution with t-butylamine.[5][134]

[edit] References
- ^ The INN originally assigned in 1974 by the World Health Organization was "amfebutamone". In 2000, the INN was reassigned as bupropion. See World Health Organization (2000). "International Nonproprietary Names for Pharmaceutical Substances (INN). Proposed INN: List 83" (PDF). WHO Drug Information 14 (2). http://82.77.46.154/gsdldata/collect/whodruginfo/index/assoc/h1463e/h1463e.pdf.
- ^ Slemmer J E, Martin R M, Damaj M I (2000). "Bupropion is a Nicotinic Antagonist". J Pharmacol Exp Ther 295 (1): 321–327.
- ^ Fryer J D, Lukas R J (1999). "Noncompetitive functional inhibition at diverse, human nicotinic acetylcholine receptor subtypes by bupropion, phencyclidine, and ibogaine". J Pharmacol Exp Ther 288 (6): 88–92. PMID 9862757.
- ^ After sertraline, escitalopram and fluoxetine. The bupropion prescriptions were calculated as a total of prescriptions for Wellbutrin XL, Budeprion XL, Budeprion SR, Bupropion SR and Bupropion ER using data from the charts for generic and brand-name drugs, see: "Top 200 Generic Drugs by Units in 2007" (PDF). Drug Topics. 2008-02-18. http://www.drugtopics.com/drugtopics/article/articleDetail.jsp?id=491181. Retrieved on 2008-03-30. and Verispan (2008-02-18). "Top 200 Brand Drugs by Units in 2007" (PDF). Drug Topics. http://www.drugtopics.com/drugtopics/article/articleDetail.jsp?id=491207. Retrieved on 2008-03-30.
- ^ a b Mehta NB (1974-06-25). "United States Patent 3,819,706: Meta-chloro substituted α-butylamino-propiophenones". USPTO. http://patft.uspto.gov/netacgi/nph-Parser?Sect1=PTO1&Sect2=HITOFF&d=PALL&p=1&u=%2Fnetahtml%2FPTO%2Fsrchnum.htm&r=1&f=G&l=50&s1=3819706.PN.&OS=PN/3819706&RS=PN/3819706. Retrieved on 2008-06-02.
- ^ WELLBUTRIN Label and Approval History. U.S. Food and Drug Administration Center for Drug Evaluation and Research. Retrieved on 2007-08-18. Data available for download on FDA website.
- ^ a b "Bupropion Helps People With Schizophrenia Quit Smoking." National Institute on Drug Abuse. Research Findings, Vol. 20, No. 5 (April 2006). Retrieved on August 19, 2007.
- ^ Staff Writer. "Seasonal affective disorder drug Wellbutrin XL wins approval." CNN. June 14, 2006. Retrieved on August 19, 2007.
- ^ Fava M, Rush AJ, Thase ME, Clayton A, Stahl SM, Pradko JF, Johnston JA. (2005). "15 years of clinical experience with bupropion HCl: from bupropion to bupropion SR to bupropion XL" (PDF). Prim Care Companion J Clin Psychiatry 7 (3): 106–113. PMID 16027765. http://www.psychiatrist.com/pcc/pccpdf/v07n03/v07n0305.pdf. Retrieved on 2008-12-30.
- ^ Thase ME, Haight BR, Richard N, Rockett CB, Mitton M, Modell JG, VanMeter S, Harriett AE, Wang Y (2005). "Remission rates following antidepressant therapy with bupropion or selective serotonin reuptake inhibitors: a meta-analysis of original data from 7 randomized controlled trials". J Clin Psychiatry 66 (6): 974–981. PMID 16086611.
- ^ Clayton AH, Croft HA, Horrigan JP, Wightman DS, Krishen A, Richard NE, Modell JG (2006). "Bupropion extended release compared with escitalopram: effects on sexual functioning and antidepressant efficacy in 2 randomized, double-blind, placebo-controlled studies". J Clin Psychiatry 67 (5): 736–746. PMID 1684162.
- ^ Thase ME, Clayton AH, Haight BR, Thompson AH, Modell JG, Johnston JA (2006). "A double-blind comparison between bupropion XL and venlafaxine XR: sexual functioning, antidepressant efficacy, and tolerability". J Clin Psychopharmacol 26 (5): 482–488. doi:. PMID 16974189.
- ^ For the review, see: Clayton AH (2003). "Antidepressant-Associated Sexual Dysfunction: A Potentially Avoidable Therapeutic Challenge". Primary Psychiatry 10 (1): 55–61.
- ^ For another review, see: Kanaly KA, Berman JR (2002). "Sexual side effects of SSRI medications: potential treatment strategies for SSRI-induced female sexual dysfunction". Curr Women's Health Rep 2 (6): 409–16. PMID 12429073.
- ^ For a short review, see: Zimmerman M, Posternak MA, Attiullah N, Friedman M, Boland RJ, Baymiller S, Berlowitz SL, Rahman S, Uy KK, Singer S, Chelminski I, Thongy, T (2005). "Dr. Zimmerman and colleagues reply to MJ Menaster". J Clin Psychiatry 66 (10): 1336–9.
- ^ Baldwin DS, Papakostas GI (2006). "Symptoms of Fatigue and Sleepiness in Major Depressive Disorder". J Clin Psychiatry 67 (suppl 6): 9–15. PMID 16848671.
- ^ Papakostas GI, Stahl SM, Krishen A, et al (July 2008). "Efficacy of Bupropion and the Selective Serotonin Reuptake Inhibitors in the Treatment of Major Depressive Disorder With High Levels of Anxiety (Anxious Depression): A Pooled Analysis of 10 Studies". J Clin Psychiatry: e1–e6. PMID 18605812. http://article.psychiatrist.com/?ContentType=START&ID=10003663.
- ^ For the most recent review, see: Zisook S, Rush AJ, Haight BR, Clines DC, Rockett CB (2006). "Use of bupropion in combination with serotonin reuptake inhibitors". Biol Psychiatry 59 (3): 203–10. doi:. PMID 16165100.
- ^ Spier SA (1998). "Use of bupropion with SRIs and venlafaxine". Depression and anxiety 7 (2): 73–5. doi:. PMID 9614595.
- ^ a b Bodkin JA, Lasser RA, Wines JD, Gardner DM, Baldessarini RJ (1997). "Combining serotonin reuptake inhibitors and bupropion in partial responders to antidepressant monotherapy". The Journal of clinical psychiatry 58 (4): 137–45. PMID 9164423.
- ^ Trivedi MH, Fava M, Wisniewski SR, Thase ME, Quitkin F, Warden D, Ritz L, Nierenberg AA, Lebowitz BD, Biggs MM, Luther JF, Shores-Wilson K, Rush AJ (2006). "Medication augmentation after the failure of SSRIs for depression". N. Engl. J. Med. 354 (12): 1243–52. doi:. PMID 16554526.
- ^ Rush AJ, Trivedi MH, Wisniewski SR, Stewart JW, Nierenberg AA, Thase ME, Ritz L, Biggs MM, Warden D, Luther JF, Shores-Wilson K, Niederehe G, Fava M (2006). "Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression". N. Engl. J. Med. 354 (12): 1231–42. doi:. PMID 16554525.
- ^ a b Tonnesen P, Tonstad S, Hjalmarson A, Lebargy F, Van Spiegel P I, Hider A, Sweet R, Townsend J (2003). "A multicentre, randomized, double-blind, placebo-controlled, 1-year study of bupropion SR for smoking cessation". J Intern Med 254 (2): 184–192. doi:. PMID 12859700.
- ^ Wu P, Wilson K, Dimoulas P, Mills E J (2006). "Effectiveness of smoking cessation therapies: a systematic review and meta-analysis". BMC Public Health 6: 300–315. doi:.
- ^ Jorenby D E, Hays J T, Rigotti N A, Azoulay S, Watsky E J, Williams K E, Billing C B, Gong J, Reeves K R (2006). "Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial". JAMA 296 (1): 56–63. doi:. PMID 16820547.
- ^ Dording CM, Mischoulon D, Petersen TJ, Kornbluh R, Gordon J, Nierenberg AA, Rosenbaum JE, Fava M. (2002). "The pharmacologic management of SSRI-induced side effects: a survey of psychiatrists". Ann Clin Psychiatry 14 (3): 143–7. doi:. PMID 12585563.
- ^ Walker PW, Cole JO, Gardner EA, Hughes AR, Johnston JA, Batey SR, Lineberry CG (1993). "Improvement in fluoxetine-associated sexual dysfunction in patients switched to bupropion". J Clin Psychiatry 54 (12): 459–65. PMID 8276736.
- ^ Dobkin RD, Menza M, Marin H, Allen LA, Rousso R, Leiblum SR (2006). "Bupropion improves sexual functioning in depressed minority women: an open-label switch study". J Clin Psychiatry 26 (1): 21–6. PMID 16415700.
- ^ Masand PS, Ashton AK, Gupta S, Frank B (2001). "Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: a randomized, double-blind, placebo-controlled, parallel-group study". Am J Psychiatry 158 (5): 805–807. doi:. PMID 11329407.
- ^ DeBattista C, Solvason B, Poirier J, Kendrick E, Loraas E (2005). "A placebo-controlled, randomized, double-blind study of adjunctive bupropion sustained release in the treatment of SSRI-induced sexual dysfunction". J Clin Psychiatry 66 (7): 844–8.
- ^ Ashton AK, Rosen RC (1998). "Bupropion as an antidote for serotonin reuptake inhibitor-induced sexual dysfunction". J Clin Psychiatry 59 (3): 112–5. PMID 9541153.
- ^ Clayton AH, Warnock JK, Kornstein SG, Pinkerton R, Sheldon-Keller A, McGarvey EL (2004). "A placebo-controlled trial of bupropion SR as an antidote for selective serotonin reuptake inhibitor-induced sexual dysfunction". J Clin Psychiatry 65 (1): 62–7. PMID 14744170.
- ^ Crenshaw TL, Goldberg JP, Stern WC (1987). "Pharmacologic modification of psychosexual dysfunction". J Sex Marital Ther 13 (4): 239–52. PMID 3121861.
- ^ Segraves RT, Croft H, Kavoussi R, Ascher JA, Batey SR, Foster VJ, Bolden-Watson C, Metz A (2001). "Bupropion sustained release (SR) for the treatment of hypoactive sexual desire disorder (HSDD) in nondepressed women". J Sex Marital Ther 27 (3): 303–16. doi:. PMID 11354935.
- ^ Segraves RT, Clayton A, Croft H, Wolf A, Warnock J. (2004). "Bupropion sustained release for the treatment of hypoactive sexual desire disorder in premenopausal women". J Clin Psychopharmacol 24 (3): 339–42. doi:. PMID 15118489.
- ^ Mathias C, Cardeal Mendes CM, Ponde de Sena E, Dias de Moraes E, Bastos C, Braghiroli MI, Nunez G, Athanazio R, Alban L, Moore HC, del Giglio A (20060). "An open-label, fixed-dose study of bupropion effect on sexual function scores in women treated for breast cancer". Ann Oncol 17 (12): 1792–6. doi:. PMID 16980597.
- ^ Modell JG, May RS, Katholi CR (2000). "Effect of bupropion-SR on orgasmic dysfunction in nondepressed subjects: a pilot study". J Sex Marital Ther 26 (3): 231–40. doi:. PMID 10929571.
- ^ Cabello F (February 2006). "Effectiveness of the Treatment of Female Hypoactive Sexual Desire Disorder". J Sex Research. http://www.findarticles.com/p/articles/mi_m2372/is_1_43/ai_n16102437. Retrieved on 2007-04-05.
- ^ Labbate LA, Brodrick PS, Nelson RP, Lydiard RB, Arana GW (2001). "Effects of bupropion sustained-release on sexual functioning and nocturnal erections in healthy men". J Clin Psychopharmacol 22 (1): 99–103. doi:. PMID 11199957.
- ^ Li Z, Maglione M, Tu W, Mojica W, Arterburn D, Shugarman LR, Hilton L, Suttorp M, Solomon V, Shekelle PG, Morton SC. (2005). "Meta-analysis: pharmacologic treatment of obesity". Ann Intern Med 142 (7): 532–46. PMID 15809465.
- ^ Wilens TE, Haight BR, Horrigan JP, Hudziak JJ, Rosenthal NE, Connor DF, Hampton KD, Richard NE, Modell JG (2005). "Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study". Biol. Psychiatry 57 (7): 793–801. doi:. PMID 15820237.
- ^ a b For the review, see: Cantwell DP (1998). "ADHD through the life span: the role of bupropion in treatment". The Journal of clinical psychiatry 59 Suppl 4: 92–4. PMID 9554326.
- ^ Steven Pliszka et al (2007). "PRACTICE PARAMETER FOR THE ASSESSMENT AND TREATMENT OF CHILDREN AND ADOLESCENTS WITH ATTENTION-DEFICIT/HYPERACTIVITY DISORDER" (PDF). American Academy of Child and Adolescent Psychiatry. 16. http://www.aacap.org/galleries/PracticeParameters/New_ADHD_Parameter.pdf. Retrieved on 2007-09-02.
- ^ Pliszka SR et al (2006). "The Texas Children's Medication Algorithm Project: attention-deficit/hyperactivity disorder.". Texas Department of State Health Services. http://www.dshs.state.tx.us/mhprograms/adhdpage.shtm. Retrieved on 2007-09-02.
- ^ "Algorithm Stages Flowsheets. ADHD with no significant comorbidity algorithm" (PDF). Texas Department of State Health Services. May 2006. http://www.dshs.state.tx.us/mhprograms/ADHD_Algo_Schematics_With_NO_Sig_Co_Dis.pdf. Retrieved on 2007-09-02.
- ^ Monuteaux MC, Spencer TJ, Faraone SV, Wilson AM, Biederman J (2007). "A randomized, placebo-controlled clinical trial of bupropion for the prevention of smoking in children and adolescents with attention-deficit/hyperactivity disorder". The Journal of clinical psychiatry 68 (7): 1094–101. PMID 17685748.
- ^ "First drug for seasonal depression". FDA Consumer 40 (5): 7. 2006. PMID 17328102.
- ^ Modell JG, Rosenthal NE, Harriett AE, Krishen A, Asgharian A, Foster VJ, Metz A, Rockett CB, Wightman DS (2005). "Seasonal affective disorder and its prevention by anticipatory treatment with bupropion XL". Biol Psychiatry 58 (8): 658–67. doi:. PMID 16271314.
- ^ For the review indicating that antidepressants are not better than placebo, see: Sachs GS, Nierenberg AA, Calabrese JR, Marangell LB, Wisniewski SR, Gyulai L, Friedman ES, Bowden CL, Fossey MD, Ostacher MJ, Ketter TA, Patel J, Hauser P, Rapport D, Martinez JM, Allen MH, Miklowitz DJ, Otto MW, Dennehy EB, Thase ME (2007). "Effectiveness of adjunctive antidepressant treatment for bipolar depression". N. Engl. J. Med. 356 (17): 1711–22. doi:. PMID 17392295.
- ^ a b For the review in favor of the antidepressant use, see: Gijsman HJ, Geddes JR, Rendell JM, Nolen WA, Goodwin GM (2004). "Antidepressants for bipolar depression: a systematic review of randomized, controlled trials". The American journal of psychiatry 161 (9): 1537–47. doi:. PMID 15337640.
- ^ For the guidelines recommending the use of bupropion with a mood stabilizer, see: Yatham LN, Kennedy SH, O'Donovan C, Parikh SV, MacQueen G, McIntyre RS, Sharma V, Beaulieu S (2006). "Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: update 2007". Bipolar Disord 8 (6): 721–39. doi:. PMID 17156158.
- ^ Goetz CG, Tanner CM, Klawans HL (1984). "Bupropion in Parkinson's disease". Neurology 34 (8): 1092–4. PMID 6431314.
- ^ American Psychiatric Association (2000). "Practice guideline for the treatment of patients with major depressive disorder. Second edition." (PDF). 37. http://www.psych.org/psych_pract/treatg/pg/MDD2e_05-15-06.pdf. Retrieved on 2007-08-24.
- ^ a b c d e f g h "Wellbutrin XL Prescribing Information" (PDF). GlaxoSmithKline. June 2006. http://us.gsk.com/products/assets/us_wellbutrinXL.pdf.
- ^ Spencer T, Biederman J, Steingard R, Wilens T (1993). "Bupropion exacerbates tics in children with attention-deficit hyperactivity disorder and Tourette's syndrome". J Am Acad Child Adolesc Psychiatry 32 (1): 211–4. PMID 8428875.
- ^ a b Levenson M, Holland C. "Antidepressants and Suicidality in Adults: Statistical Evaluation. (Presentation at Psychopharmacologic Drugs Advisory Committee; December 13, 2006)". http://www.fda.gov/ohrms/dockets/ac/06/slides/2006-4272s1-04-FDA.ppt. Retrieved on 2007-05-13.
- ^ Hughes JR, Stead LF, Lancaster T (2007). "Antidepressants for smoking cessation". Cochrane Database Syst Rev. 24 (1): CD000031. doi:. PMID 17253443.
- ^ Pisani F, Oteri G, Costa C, Di Raimondo G, Di Perri R (2002). "Effects of Psychotropic Drugs on Seizure Threshold". Drug Safety 25 (2): 91–110. doi:.
- ^ Ahern TH, Javors MA, Eagles DA, Martillotti J, Mitchell HA, Liles LC, Weinshenker D (2006). "The effects of chronic norepinephrine transporter inactivation on seizure susceptibility in mice". Neuropsychopharmacology 31 (4): 730–8. doi:. PMID 16052243.
- ^ Alper K, Schwartz KA, Kolts RL, Khan A (2007). "Seizure Incidence in Psychopharmacological Clinical Trials: An Analysis of Food and Drug Administration (FDA) Summary Basis of Approval Reports". Biol Psychiatry 62 (4): 345–54. doi:. PMID 17223086.
- ^ Post RM, Altshuler LL, Leverich GS, Frye MA, Nolen WA, Kupka RW, Suppes T, McElroy S, Keck PE, Denicoff KD, Grunze H, Walden J, Kitchen CM, Mintz J (2006). "Mood switch in bipolar depression: comparison of adjunctive venlafaxine, bupropion and sertraline". Br J Psychiatry 189: 124–31. PMID 16880481.
- ^ Roose SP, Dalack GW, Glassman AH, Woodring S, Walsh BT, Giardina EG (1991). "Cardiovascular effects of bupropion in depressed patients with heart disease". Am J Psychiatry 148 (4): 512–6. PMID 1900980.
- ^ Aubin HJ (2002). "Tolerability and safety of sustained-release bupropion in the management of smoking cessation". Drugs 62 Suppl 2: 45–52. PMID 12109935.
- ^ Wilens TE, Hammerness PG, Biederman J, Kwon A, Spencer TJ, Clark S, Scott M, Podolski A, Ditterline JW, Morris MC, Moore H (2005). "Blood pressure changes associated with medication treatment of adults with attention-deficit/hyperactivity disorder". J Clin Psychiatry 66 (2): 253–9. PMID 15705013.
- ^ Rigotti NA, Thorndike AN, Regan S, McKool K, Pasternak RC, Chang Y, Swartz S, Torres-Finnerty N, Emmons KM, Singer DE (2006). "Bupropion for smokers hospitalized with acute cardiovascular disease". Am J Med 119 (12): 1080–7. doi:. PMID 17145253.
- ^ van Melle JP, de Jonge P, van den Berg MP, Pot HJ, van Veldhuisen DJ (2006). "Treatment of depression in acute coronary syndromes with selective serotonin reuptake inhibitors". Drugs 66 (16): 2095–107. PMID 17112303.
- ^ "Zyban (bupropion hydrochloride) – safety update". Medicines and Healthcare products Regulatory Agency. 2002-07-24. http://www.mhra.gov.uk/home/idcplg?IdcService=GET_FILE&dID=2556&noSaveAs=0&Rendition=WEB. Retrieved on 2006-10-07.
- ^ Hubbard R, Lewis S, West J, Smith C, Godfrey C, Smeeth L, Farrington P, Britton J (2005). "Bupropion and the risk of sudden death: a self-controlled case-series analysis using The Health Improvement Network". Thorax 60 (10): 848–50. doi:. PMID 16055620. Free full text
- ^ Wang, Hy; Chou, Wj; Huang, Ty; Hung, Cf (April 2007). "Acute dystonia resulting from abrupt bupropion discontinuation". Progress in neuro-psychopharmacology & biological psychiatry 31 (3): 766–8. doi:. PMID 17218049.
- ^ Berigan, Tr (April 2002). "Bupropion-Associated Withdrawal Symptoms Revisited: A Case Report". Primary care companion to the Journal of clinical psychiatry 4 (2): 78. ISSN 1523-5998. PMID 15014751. PMC: 181231. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=15014751.
- ^ Berigan, Tr; Harazin, Js (April 1999). "Bupropion-Associated Withdrawal Symptoms: A Case Report". Primary care companion to the Journal of clinical psychiatry 1 (2): 50–51. ISSN 1523-5998. PMID 15014696. PMC: 181057. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=15014696.
- ^ Michael, N; Erfurth, A; Bergant, V (February 2004). "A case report of mania related to discontinuation of bupropion therapy for smoking cessation". The Journal of clinical psychiatry 65 (2): 277. ISSN 0160-6689. PMID 15003088.
- ^ For the most recent report, see: Alvaro D, Onetti-Muda A, Moscatelli R, Atili AF (2001). "Acute cholestatic hepatitis induced by bupropion prescribed as pharmacological support to stop smoking. A case report". Digestive and liver disease 33 (8): 703–6. doi:. PMID 11785718.
- ^ Levenson JL (1995). "Priapism associated with bupropion treatment". Am J Psychiatry 152 (5): 813. PMID 7726332.
- ^ a b c d Balit CR, Lynch CN, Isbister GK (2003). "Bupropion poisoning: a case series". Med. J. Aust. 178 (2): 61–3. PMID 12526723.
- ^ a b c d e Buckley NA, Faunce TA (2003). "'Atypical' antidepressants in overdose: clinical considerations with respect to safety". Drug safety: an international journal of medical toxicology and drug experience 26 (8): 539–51. PMID 12825968.
- ^ a b Spiller HA, Ramoska EA, Krenzelok EP, Sheen SR, Borys DJ, Villalobos D, Muir S, Jones-Easom L (1994). "Bupropion overdose: a 3-year multi-center retrospective analysis". The American journal of emergency medicine 12 (1): 43–5. doi:. PMID 8285970.
- ^ Mainie I, McGurk C, McClintock G, Robinson J (2001). "Seizures after buproprion overdose". Lancet 357 (9268): 1624. doi:. PMID 11386326.
- ^ a b Shepherd G, Velez LI, Keyes DC (2004). "Intentional bupropion overdoses". The Journal of emergency medicine 27 (2): 147–51. doi:. PMID 15261357.
- ^ Curry SC, Kashani JS, LoVecchio F, Holubek W (2005). "Intraventricular conduction delay after bupropion overdose". The Journal of emergency medicine 29 (3): 299–305. doi:. PMID 16183450.
- ^ Tracey JA, Cassidy N, Casey PB, Ali I (2002). "Bupropion (Zyban) toxicity". Irish medical journal 95 (1): 23–4. PMID 11928786.
- ^ Shepherd G, Velez LI, James DK, Keyes DC (2001). "Pediatric bupropion exposures reported in Texas: 1998–1999 [abstract]". J Toxicol Clin Toxicol 39: 263.
- ^ Colbridge MG, Dargan PI, Jones AL (2002). "Bupropion - the experience of the National Poisons Information Service (London) [abstract]". J Toxicol Clin Toxicol 40: 398–9.
- ^ Johnston JA, Lineberry CG, Ascher JA, Davidson J, Khayrallah MA, Feighner JP, Stark P (1991). "A 102-center prospective study of seizure in association with bupropion". The Journal of clinical psychiatry 52 (11): 450–6. PMID 1744061.
- ^ Harris CR, Gualtieri J, Stark G (1997). "Fatal bupropion overdose". J Toxicol Clin Toxicol 35 (3): 321–4. PMID 9140330.
- ^ Friel PN, Logan BK, Fligner CL (1993). "Three fatal drug overdoses involving bupropion". Journal of analytical toxicology 17 (7): 436–8. PMID 8309220.
- ^ Paoloni R, Szekely I (2002). "Sustained-release bupropion overdose: a new entity for Australian emergency departments". Emergency medicine (Fremantle, W.A.) 14 (1): 109–12. doi:. PMID 11993828.
- ^ Sirianni AJ, Osterhoudt KC, Calello DP, et al (2007). "Use of Lipid Emulsion in the Resuscitation of a Patient With Prolonged Cardiovascular Collapse After Overdose of Bupropion and Lamotrigine". Ann Emerg Med 51: 412. doi:. PMID 17766009.
- ^ Stahl S, Pradko J, Haight B, Modell J, Rockett C, Learned-Coughlin S (2004). "A Review of the Neuropharmacology of Bupropion, a Dual Norepinephrine and Dopamine Reuptake Inhibitor" (PDF). Prim Care Companion J Clin Psychiatry 6 (4): 159–166. PMID 15361919. http://www.psychiatrist.com/pcc/pccpdf/v06n04/v06n0403.pdf. Retrieved on 2008-12-30. Full text at PMC: 514842
- ^ Meyer J, Goulding V S, Wilson A A, Hussey D, Christensen B K, Houle S (2002). "Bupropion occupancy of the dopamine transporter is low during clinical treatment". Psychopharmacology 163: 102–105. doi:. PMID 12185406.
- ^ Learned-Coughkin S M, Bergstrom M, Savitcheva I, Ascher J, Schmith V D, Langstrom B (2003). "In vivo activity of bupropion at the human dopamine transporter as measured by positron emission tomography". Biol Psychiatry 54: 800–805. doi:. PMID 14550679.
- ^ Fryer J D, Lukas R J (1999). "Noncompetitive functional inhibition at diverse, human nicotinic acetylcholine receptor subtypes by bupropion, phencyclidine, and ibogaine". J Pharmacol Exp Ther 288 (6): 88–92. PMID 9862757.
- ^ Glick S D. "Ibogaine Analogues: Drug Development for Addictive Disorders. (Presentation at Addiction Medicine State of the Art 2003 Conference October 8–11, 2003, Radisson-Miyako Hotel, San Francisco)". www.csam-asam.org. http://www.csam-asam.org/pdf/misc/Glick.ppt. Retrieved on 2007-03-24.
- ^ Physicians' Desk Reference (59 ed.). Montvale, NJ: Thompson. 2005. ISBN 1-56363-497-X.
- ^ a b Horst WD, Preskorn SH (1998). "Mechanisms of action and clinical characteristics of three atypical antidepressants: venlafaxine, nefazodone, bupropion". J Affect Disord 51 (3): 237–54. doi:. PMID 10333980.
- ^ PRNewswire (November 23, 2004). GlaxoSmithKline (GSK) Reviews Novel Therapeutics For CNS Disorders And Confirms Strong Pipeline Momentum. Press release. http://www.biospace.com/news_story.aspx?StoryID=18222420&full=1. Retrieved on 2007-08-18.
- ^ GlaxoSmithKline (July 26, 2006) Pipeline UpdatePDF (136 KB). Press release. Retrieved on 2007-08-18.
- ^ Kirchheiner J, Klein C, Meineke I, Sasse J, Zanger UM, Mürdter TE, Roots I, Brockmöller J (2003). "Bupropion and 4-OH-bupropion pharmacokinetics in relation to genetic polymorphisms in CYP2B6". Pharmacogenetics 13 (10): 619–26. doi:. PMID 14515060.
- ^ Hesse LM, He P, Krishnaswamy S, Hao Q, Hogan K, von Moltke LL, Greenblatt DJ, Court MH (2004). "Pharmacogenetic determinants of interindividual variability in bupropion hydroxylation by cytochrome P450 2B6 in human liver microsomes". Pharmacogenetics 14 (4): 225–38. doi:. PMID 15083067.
- ^ Preskorn SH (1991). "Should bupropion dosage be adjusted based upon therapeutic drug monitoring?". Psychopharmacology bulletin 27 (4): 637–43. PMID 1813908.
- ^ Suckow R F, Smith T M, Perumal A S, Cooper T B (1986). "Pharmacokinetics of bupropion and metabolites in plasma and brain of rats, mice, and guinea pigs". Drug Metab Dispos 14 (6): 692–697. PMID 2877828.
- ^ a b Welch R M, Lai A A, Schroeder D H (1987). "Pharmacological significance of the species differences in bupropion metabolism". Xenobiotica 17 (3): 287–289. PMID 3107223.
- ^ Weintraub D, Linder MW (2000). "Amphetamine positive toxicology screen secondary to bupropion". Depress Anxiety 12 (1): 53–4. doi:. PMID 10999247.
- ^ Nixon AL, Long WH, Puopolo PR, Flood JG (1995). "Bupropion metabolites produce false-positive urine amphetamine results". Clin. Chem. 41 (6 Pt 1): 955–6. PMID 7768026.
- ^ Johnston AJ, Ascher J, Leadbetter R, Schmith VD, Patel DK, Durcan M, Bentley B (2002). "Pharmacokinetic optimisation of sustained-release bupropion for smoking cessation". Drugs 62 (Suppl 2): 11–24. doi:. PMID 12109932.
- ^ Xu H, Loboz KK, Gross AS, McLachlan AJ (2007). "Stereoselective analysis of hydroxybupropion and application to drug interaction studies". Chirality 19 (3): 163–70. doi:. PMID 17167747.
- ^ Bondarev ML, Bondareva TS, Young R, Glennon RA (2003). "Behavioral and biochemical investigations of bupropion metabolites". Eur J Pharmacol 474 (1): 85–93. doi:. PMID 12909199.
- ^ Damaj MI, Carroll FI, Eaton JB, Navarro HA, Blough BE, Mirza S, Lukas RJ, Martin BR (2004). "Enantioselective effects of hydroxy metabolites of bupropion on behavior and on function of monoamine transporters and nicotinic receptors". Mol Pharmacol 66 (3): 675–82. doi:. PMID 15322260.
- ^ a b Jefferson JW, Pradko JF, Muir KT (2005). "Bupropion for major depressive disorder: Pharmacokinetic and formulation considerations". Clin Ther 27 (11): 1685–95. doi:. PMID 16368442.
- ^ Kennedy SH, McCann SM, Masellis M, McIntyre RS, Raskin J, McKay G, Baker GB (2002). "Combining bupropion SR with venlafaxine, paroxetine, or fluoxetine: a preliminary report on pharmacokinetic, therapeutic, and sexual dysfunction effects". J Clin Psychiatry 63 (3): 181–6. PMID 11926715.
- ^ "P02-31UK I Examination of Bupropion and Ethanol, Alone and in Combination, on Human Performance Tests, Subjective Rating Scales, EEG and Autonomic Responses" (PDF). GlaxoSmithKline Clinical Trial Register. Bupropion Studies. http://ctr.gsk.co.uk/Summary/bupropion/I_031.pdf. Retrieved on 2007-06-04.
- ^ "Practitioner's Reporting News". United States Pharmacopeia. 2004-09-30. http://www.usp.org/hqi/practitionerPrograms/newsletters/practitionerReportingNews/prn1202004-09-30.html#14. Retrieved on 2007-08-20.
- ^ Rosack, Jim (2006-03-17). "Company Tries to Clear Up Confusion About Bupropion". Psychiatric News (American Psychiatric Association) 41 (6): 16. http://pn.psychiatryonline.org/cgi/content/full/41/6/16. Retrieved on 2007-08-20.
- ^ "BuPROPion: Drug Information Provided by Lexi-Comp: Merck Manual Professional". http://www.merck.com/mmpe/print/lexicomp/bupropion.html. Retrieved on 2007-06-16.
- ^ Waknine, Yael (2008-05-08). "FDA Approvals: Advair, Relistor, Aplenzin". Medscape. http://www.medscape.com/viewarticle/574187. Retrieved on 2008-05-09.
- ^ "Generic Drug Equality Questioned". http://www.peoplespharmacy.com/archives/generic_drug_problems/generic_drug_equality_questioned.php. Retrieved on 2007-10-13.
- ^ Jacqueline Stenson (2007-10-12). "Report questions generic antidepressant - Health Care - MSNBC.com". MSNBC. http://www.msnbc.msn.com/id/21142869/. Retrieved on 2007-10-13.
- ^ "Review of Therapeutic Equivalence: Generic Bupropion XL 300 mg and Wellbutrin XL 300 mg". http://www.fda.gov/cder/drug/infopage/bupropion/TE_review.htm. Retrieved on 2008-04-19.
- ^ Agence française de sécurité sanitaire des produits de santé (January 18, 2001) (in French). ZYBAN : sevrage tabagique et sécurité d’emploi. Press release. http://afssaps.sante.fr/htm/10/filcoprs/020102c.htm. Retrieved on 2007-08-19.
- ^ GlaxoSmithKline (2007-01-16). GlaxoSmithKline receives first European approval for Wellbutrin XR. Press release. http://www.gsk.com/ControllerServlet?appId=4&pageId=402&newsid=956. Retrieved on 2007-08-19.
- ^ "Exhibit 4-3 Abuse Potential of Common Psychiatric Medications". Health Services/Technology Assessment Text (HSTAT). U.S. National Library of Medicine. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.table.36258. Retrieved on 2007-05-25.
- ^ "Figure 3-4: Abuse Potential of Common Psychiatric Medications". Health Services/Technology Assessment Text (HSTAT). U.S. National Library of Medicine. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.table.67504. Retrieved on 2007-05-25.
- ^ Bergman J, Madras BK, Johnson SE, Spealman RD (1989). "Effects of cocaine and related drugs in nonhuman primates. III. Self-administration by squirrel monkeys". J. Pharmacol. Exp. Ther. 251 (1): 150–5. PMID 2529365.
- ^ Tella SR, Ladenheim B, Cadet JL (1997). "Differential regulation of dopamine transporter after chronic self-administration of bupropion and nomifensine". J Pharmacol Exp Ther 281 (1): 508–13. PMID 9103538.
- ^ Miller L, Griffith J (1983). "A comparison of bupropion, dextroamphetamine, and placebo in mixed-substance abusers". Psychopharmacology (Berl.) 80 (3): 199–205. doi:. PMID 6412263.
- ^ Griffith JD, Carranza J, Griffith C, Miller LL (1983). "Bupropion: clinical assay for amphetamine-like abuse potential". J Clin Psychiatry 44 (5 Pt 2): 206–8. PMID 6406459.
- ^ Rush CR, Kollins SH, Pazzaglia PJ (1998). "Discriminative-stimulus and participant-rated effects of methylphenidate, bupropion, and triazolam in d-amphetamine-trained humans". Experimental and clinical psychopharmacology 6 (1): 32–44. doi:. PMID 9526144.
- ^ Zernig G, De Wit H, Telser S, et al (2004). "Subjective effects of slow-release bupropion versus caffeine as determined in a quasi-naturalistic setting". Pharmacology 70 (4): 206–15. doi:. PMID 15001822.
- ^ Khurshid KA, Decker DH (2004). "Bupropion insufflation in a teenager". J Child Adolesc Psychopharmacol 14 (1): 157–8. doi:. PMID 15142406.
- ^ Lu JJ, Thompson TM, Narunatvanich D, Fischbein CB, Mycyk MB (2007). "Seizure after Nasal Insufflation of Bupropion [abstract]". Clin Toxicol (Phila) 45: 632.
- ^ Welsh CJ, Doyon S (2002). "Seizure induced by insufflation of bupropion". N. Engl. J. Med. 347 (12): 951. doi:. PMID 12239274.
- ^ McCormick J (2002). "Recreational bupropion abuse in a teenager". Br J Clin Pharmacol 53 (2): 214. doi:. PMID 11851650.
- ^ Volpe KD. "Intervention Reduces Psychotropic Abuse in Correctional Facility; CNS News, JUNE 2005, VOLUME: 07:06". http://www.cnsnewsonline.com/index.asp?section_id=113&show=dept&article_id=4907. Retrieved on 2007-05-27.
- ^ Daniel M. Perrine, Jason T. Ross, Stephen J. Nervi, and Richard H. Zimmerman (2000). "A Short, One-Pot Synthesis of Bupropion". J. Chem. Ed. 77 (11): 1479. http://jchemed.chem.wisc.edu/Journal/Issues/2000/nov/PlusSub/V77N11/p1479.pdf.
[edit] External links
- Wellbutrin official website
- List of international brand names for bupropion
- Bupropion at the Open Directory Project
- Wellbutrin Pharmacology, Pharmacokinetics, Studies, Metabolism - Bupropion - RxList Monographs
- NAMI Wellbutrin
- Bupropion article from mentalhealth.com
|
|||||
|
|||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||
|
|||||||||||

