Tobacco smoking
From Wikipedia, the free encyclopedia
Tobacco · Demographics · Health
Industry · Politics · Advertising
Opium poppy · Opiate · Opioid
Den · Wars · Psychoactive drug
Tobacco smoking is the practice where the substance, tobacco, is burned (pyrolyzed) and the vapors either tasted or inhaled. The practice dates back to 5000 BC in shamanistic rituals.[1][2] Many civilizations burnt incense as part of their religious rituals, which was later adopted for pleasure or as a social tool.[3] Tobacco was introduced to the old world in the late 1500s where it followed common trade routes. The substance was met with frequent criticism, however it became popular nonetheless.[4] The industrialization of production and increased life expectancies in the late 1920s prompted anti-smoking groups to advocacate against its usage. This movement was in Nazi Germany, however following the Second World War health research in Germany was described as "muted".[5] It was not until the late 1950s before health authorities began suggest the relationship between smoking and cancer.[6] These suggestions were confirmed in the 1980s, which prompted political action against the practice. Rates of consumption from 1965 onward in the developed world have either peaked or declined.[7] They however continue to climb in the developing world.[8]
Smoking is the most common method of consuming tobacco. Tobacco is likewise the most common substance smoked. The argicultural product is often mixed with other additives[9] and then pyrolyzed. The resulting vapors are then inhaled and the active substances absorbed through the alveoli in the lungs.[10] The active substances trigger chemical reactions in nerve endings which hightens heart rate, memory, altertness,[11] and reaction time.[12] Dopamine and later endorphins are released, which are often assoicated with reward and pleasure.[13] As of 2000, smoking is practiced by some 1.22 billion people, of which men are more likely to smoke than women,[14] however the gender gap declines with age,[15][16] poor more likely than rich, and people of developing countries than those of developed countries.[8]
Many smokers begin during adolescence or early adulthood. During the early stages, smoking provides pleasurable sensations and thus serves as a source of positive reinforcement. After an individual has smoked for many years, the avoidance of withdrawal symptoms and negative reinforcement become the key motivations.
Contents |
History
Early use

The history of smoking dates back to as early as 5000 BC in shamanistic rituals.[1][2][page needed] Many ancient civilizations, such as the Babylonians, Indians and Chinese, burnt incense as a part of religious rituals, as did the Israelites and the later Catholic and Orthodox Christian churches. Smoking in the Americas probably had its origins in the incense-burning ceremonies of shamans but was later adopted for pleasure or as a social tool.[3] The smoking of tobacco and various other hallucinogenic drugs was used to achieve trances and to come into contact with the spirit world.
Eastern North American tribes would carry large amounts of tobacco in pouches as a readily accepted trade item and would often smoke it in pipes, either in defined ceremonies that were considered sacred, or to seal a bargain,[17] and they would smoke it at such occasions in all stages of life, even in childhood.[18][page needed] It was believed that tobacco was a gift from the Creator and that the exhaled tobacco smoke was capable of carrying one's thoughts and prayers to heaven.[19]
Apart from smoking, tobacco had a number of uses as medicine. As a pain killer it was used for earache and toothache and occasionally as a poultice. Smoking was said by the desert Indians to be a cure for colds, especially if the tobacco was mixed with the leaves of the small Desert Sage, Salvia Dorrii, or the root of Indian Balsam or Cough Root, Leptotaenia multifida, the addition of which was thought to be particularly good for asthma and tuberculosis.[20]
Popularization

In 1612, six years after the settlement of Jamestown, John Rolfe was credited as the first settler to successfully raise tobacco as a cash crop. The demand quickly grew as tobacco, referred to as "brown gold", reviving the Virginia join stock company from its failed gold expeditions.[21] In order to meet demands from the old world, tobacco was grown in succession, quickly depleting the land. This became a motivator to settle west into the unknown continent, and likewise an expansion of tobacco production.[22] Indentured servitude became the primary labor force up until Bacon's Rebellion, from which the focus turned to slavery.[23] This trend abated following the American revolution as slavery became regarded as unprofitable. However the practice was revived in 1794 with the invention of the cotton gin.[24][page needed]
A Frenchman named Jean Nicot (from whose name the word nicotine is derived) introduced tobacco to France in 1560. From France tobacco spread to England. The first report of a smoking Englishman is of a sailor in Bristol in 1556, seen "emitting smoke from his nostrils".[4] Like tea, coffee and opium, tobacco was just one of many intoxicants that was originally used as a form of medicine.[25] Tobacco was introduced around 1600 by French merchants in what today is modern-day Gambia and Senegal. At the same time caravans from Morocco brought tobacco to the areas around Timbuktu and the Portuguese brought the commodity (and the plant) to southern Africa, establishing the popularity of tobacco throughout all of Africa by the 1650s.
Soon after its introduction to the Old World, tobacco came under frequent criticism from state and religious leaders. Murad IV, sultan of the Ottoman Empire 1623-40 was among the first to attempt a smoking ban by claiming it was a threat to public moral and health. The Chinese emperor Chongzhen issued an edict banning smoking two years before his death and the overthrow of the Ming dynasty. Later, the Manchu of the Qing dynasty, who were originally a tribe of nomadic horse warriors, would proclaim smoking "a more heinous crime than that even of neglecting archery". In Edo period Japan, some of the earliest tobacco plantations were scorned by the shogunate as being a threat to the military economy by letting valuable farmland go to waste for the use of a recreational drug instead of being used to plant food crops.[26]

Religious leaders have often been prominent among those who considered smoking immoral or outright blasphemous. In 1634 the Patriarch of Moscow forbade the sale of tobacco and sentenced men and women who flaunted the ban to have their nostrils slit and their backs whipped until skin came off their backs. The Western church leader Urban VII likewise condemned smoking in a papal bull of 1642. Despite many concerted efforts, restrictions and bans were almost universally ignored. When James I of England, a staunch anti-smoker and the author of a A Counterblaste to Tobacco, tried to curb the new trend by enforcing a whopping 4000% tax increase on tobacco in 1604, it proved a failure, as London had some 7,000 tobacco sellers by the early 1600s. Later, scrupulous rulers would realise the futility of smoking bans and instead turned tobacco trade and cultivation into lucrative government monopolies.[27][28]
By the mid-1600s every major civilization had been introduced to tobacco smoking and in many cases had already assimilated it into the native culture, despite the attempts of many rulers to stamp the practice out with harsh penalties or fines. Tobacco, both product and plant, followed the major trade routes to major ports and markets, and then on into the hinterlands. The English language term smoking was coined in the late 1700s, before then the practice was referred to as drinking smoke.[4][page needed]
The growth remained stable until the American Civil War in 1860s, from which the primary labor force transition from slavery to share cropping. This compounded with a change in demand, lead to the industrialization of tobacco production with the cigarette. James Bonsack, a craftsman, in 1881 produce a machine to speed the production in cigarettes.[29]
Social stigma

With the modernization of cigarette production compounded with the increased life expectancies during the 1920s, adverse health effects began to become more prevalent. In Germany, anti-smoking groups, often associated with anti-liquor groups,[30] first published advocacy against the consumption of tobacco in the journal Der Tabakgegner (The Tobacco Opponent) in 1912 and 1932. In 1929, Fritz Lickint of Dresden, Germany, published a paper containing formal statistical evidence of a lung cancer–tobacco link. During the Great depression Adolf Hitler condemned his earlier smoking habit as a waste of money,[31] and later with stronger assertions. This movement was further strengthened with Nazi reproductive policy as women who smoked were viewed as unsuitable to be wives and mothers in a German family.[32]
The movement in Nazi Germany did not reach across enemy lines during the Second World War, as anti-smoking groups quickly lost popular support. By the end of the Second World War, American cigarette manufactures quickly reentered the German black market. Illegal smuggling of tobacco became prevalent,[33] and leaders of the Nazi anti-smoking campaign were assassinated.[34] As part of the Marshall Plan, the United States shipped free tobacco to Germany; with 24,000 tons in 1948 and 69,000 tons in 1949.[33] Per capita yearly cigarette consumption in post-war Germany steadily rose from 460 in 1950 to 1,523 in 1963.[5] By the end of the 1900s, anti-smoking campaigns in Germany was unable to exceed the effectiveness of the Nazi-era climax in the years 1939–41 and German tobacco health research was described by Robert N. Proctor as "muted".[5]
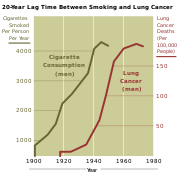
Richard Doll in 1950 published research in the British Medical Journal showing a close link between smoking and lung cancer.[35] Four years later, in 1954 the British Doctors Study, a study of some 40 thousand doctors over 20 years, confirmed the suggestion, based on which the government issued advice that smoking and lung cancer rates were related.[6] In 1964 the United States Surgeon General's Report on Smoking and Health likewise began suggesting the relationship between smoking and cancer, which confirmed its suggestions 20 years later in the 1980s.
As scientific evidence mounted in the 1980s, tobacco companies claimed contributory negligence as the adverse health effects were previously unknown or lacked substantial credibility. Health authorities sided with these claims up until 1998, from which they reversed their position. The Tobacco Master Settlement Agreement, originally between the four largest US tobacco companies and the Attorneys General of 46 states, restricted certain types of tobacco advertisement and required payments for health compensation; which later amounted to the largest civil settlement in United States history.[36]
From 1965 to 2006, rates of smoking in the United States have declined from 42% to 20.8%.[7] The significant majority of those who quit in were professional, affluent men. Despite this decrease in the prevalence of consumption, the average number of cigarettes consumed per person per day increased from 22 in 1954 to 30 in 1978. This paradoxical event suggests that those who quit smoked less, while those who continued to smoke moved to smoke more light cigarettes.[37] This trend has been paralleled by many industrialized nations as rates have either leveled-off or declined. In the developing world, however, tobacco consumption continues to rise at 3.4% in 2002.[8] In Africa, smoking is in most areas considered to be modern, and many of the strong adverse opinions that prevail in the West receive much less attention.[38] Today Russia leads as the top consumer of tobacco followed by Indonesia, Laos, Ukraine, Belarus, Greece, Jordan, and China.[39] The World Health Organization has begun a program known as the Tobacco Free Initiative (TFI) in order to reduce rates of consumption in the developing world.
Consumption
Methods
Tobacco is an agricultural product processed from the fresh leaves of plants in the genus Nicotiana. The genus contains a number of species, however, Nicotiana tabacum is the commonly grown. Nicotiana rustica follows as second and generally contain higher concentrations of nicotine. These leaves are harvested and cured to allow for the slow oxidation and degradation of carotenoids in tobacco leaf. This produces certain compounds in the tobacco leaves which can be attributed to sweet hay, tea, rose oil, or fruity aromatic flavors. Before packaging, the tobacco is often combined with other additives in order to: enhance the addictive potency, shift the products pH, or improve the effects of smoke by making it more palatable. In the United States these additives are regulated to a set number of 599 substances.[9] The product is then processed, packaged, and shipped to consumer markets.
- Beedi
- Beedis are thin, often flavored, South Asian cigarette made of tobacco wrapped in a tendu leaf, and secured with colored thread at one end.[citation needed] Bidis smoke produce higher levels of carbon monoxide, nicotine, and tar than cigarettes typical in the United States.[40][41] Due to the relatively low cost of beedies compared with regular cigarettes, they have long been popular among the poor in Bangladesh, Pakistan, Sri Lanka, Cambodia and India.[citation needed]
- Cigars
- Cigars are tightly rolled bundle of dried and fermented tobacco which is ignited so that its smoke may be drawn into the smoker's mouth. They are generally not inhaled because the high alkalinity of the smoke, which can quickly become irritating to the trachea and lungs. Instead they are generally drawn into the mouth.[citation needed] The prevalence of cigar smoking varies depending on location, historical period, and population surveyed, and prevalence estimates vary somewhat depending on the survey method. The United States is the top consuming country by far, followed by Germany and the United Kingdom; the US and Western Europe account for about 75% of cigar sales worldwide.[42] As of 2005 it is estimated that 4.3% of men and 0.3% of women smoke cigars.[43]
- Cigarettes
- Cigarettes, French for "small cigar", are a product consumed through smoking and manufactured out of cured and finely cut tobacco leaves and reconstituted tobacco, often combined with other additives, which are then rolled or stuffed into a paper-wrapped cylinder.[9] Cigarettes are ignited and inhaled, usually through a cellulose acetate filter, into the mouth and lungs. Cigarette smoking is the most common method of consumption.[citation needed]
- Electronic cigarette
- Electronic cigarettes is an alternative to tobacco smoking, although no tobacco is consumed. It is a battery-powered device that provides inhaled doses of nicotine by delivering a vaporized propylene glycol/nicotine solution. Many legislation and public health investigations are currently pending in many countries due to its relatively recent emergence.
- Hookah
- Hookah are a single or multi-stemmed (often glass-based) water pipe for smoking. Originally from India, the hookah has gained immense popularity, especially in the middle east. A hookah operates by water filtration and indirect heat. It can be used for smoking herbal fruits, tobacco, or cannabis.
- Kreteks
- Kreteks are cigarettes made with a complex blend of tobacco, cloves and a flavoring "sauce". It was first introduced in the 1880s in Kudus, Java, to deliver the medicinal eugenol of cloves to the lungs. The quality and variety of tobacco play an important role in kretek production, from which kreteks can contain more than 30 types of tobacco. Minced dried clove buds weighing about 1/3 of the tobacco blend are added to add flavouring. Several states in the United States have baned Kreteks,[citation needed] and in 2004 the United States prohibited cigarettes from having a "characterising flavor" of certain ingredients other than tobacco and menthol, thereby removing Kreteks from being classified as cigarettes.[44]
- Passive smoking
- Passive smoking is the involuntary consumption of smoked tobacco. Second-hand smoke (SHS) is the consumption where the burning end is present, environmental tobacco smoke (ETS) or third-hand smoke is the consumption of the smoke that remains after the burning end has been extinguished. Because of its negative implications, this form of consumption has played a central role in the regulation of tobacco products.
- Pipe smoking
- Pipe smoking typically consists of a small chamber (the bowl) for the combustion of the tobacco to be smoked and a thin stem (shank) that ends in a mouthpiece (the bit). Shredded pieces of tobacco are placed into the chamber and ignited. Tobaccos for smoking in pipes are often carefully treated and blended to achieve flavour nuances not available in other tobacco products.
- Roll-Your-Own
- Roll-Your-Own or hand-rolled cigarettes, are very popular particularly in European countries. These are prepared from loose tobacco, cigarette papers and filters all bought separately. They are usually much cheaper to make.
Physiology

The active substances can be administered by hypodermic injection, transdermal patches, eye droplets, nasal sprays, oral consumption, topical application, or inhalation by either finely grinding the substance or by burning it. Inhaling a vaporized gas quickly and effectively delivers substances into the bloodstream by absorption through the alveoli in the lungs. The lungs contain some 300 million alveoli, which amounts to a surface area of over 70 m2 (about the size of a tennis court). This method is somewhat inefficient as not all of the smoke will be inhaled, and some amount of the active substances will be lost in the process of combustion (pyrolysis).[10]
The inhaled substances trigger chemical reactions in nerve endings. The cholinergic receptors are often triggered by the naturally occurring substance acetylcholine. Acetylcholine and Nicotine express chemical similarities, which allows Nicotine to tigger the receptor as well. These nicotinic acetylcholine receptors takes part in two major types of neurotransmission, synaptic transmission and paracrine signalling.[45] This activity increases hearth rate, memory, alertness,[11] and produces a measurably faster reaction time after subjects have smoked.[12] Dopamine and later endorphins are released, which are associated with sensations of pleasure and reward.[13]
When tobacco is smoked, most of the nicotine is pyrolyzed. However, a dose sufficient to cause mild somatic dependency and mild to strong psychological dependency remains. There is also a formation of harmane (a MAO inhibitor) from the acetaldehyde in tobacco smoke. This seems to play an important role in nicotine addiction—probably by facilitating a dopamine release in the nucleus accumbens as a response to nicotine stimuli.[46]
Demographics

![Percentage of males smoking any tobacco product. Note that there is a difference between the scales used for females and the scales used for males.[47]](http://upload.wikimedia.org/wikipedia/commons/thumb/1/1b/Male_Smoking_by_Country.png/250px-Male_Smoking_by_Country.png)
As of 2000, smoking is practiced by 1.22 billion people. Assuming no change in prevalence it is predicted that 1.45 billion people will smoke in 2010 and 1.5 to 1.9 billion in 2025. Assuming that prevalence will decrease at 1% a year and that there will be a modest increase of income of 2%, it is predicted the number of smokers will stand at 1.3 billion in 2010 and 2025.[14]
Smoking is generally five times higher among men than women,[14] however the gender gap declines with younger age.[15][16] In developed countries smoking rates for men have peaked and have begun to decline, however for women they continue to climb.[48]
As of 2002, about twenty percent of young teens (13–15) smoke worldwide. From which 80,000 to 100,000 children begin smoking every day—roughly half of which live in Asia. Half of those who begin smoking in adolescent years are projected to go on to smoke for 15 to 20 years.[8]
The World Health Organization (WHO) states that "Much of the disease burden and premature mortality attributable to tobacco use disproportionately affect the poor". Of the 1.22 billion smokers, 1 billion of them live in developing or transitional economies. Rates of smoking have leveled off or declined in the developed world.[49] In the developing world, however, tobacco consumption is rising by 3.4% per year as of 2002.[8]
The WHO in 2004 projected 58.8 million deaths to occur globally,[50] from which 5.4 million are tobacco-attributed,[51] and 4.9 million as of 2007.[52] As of 2002, 70% of the deaths are in developing countries.[52]
Psychology
Takeup
Most smokers begin during adolescence or early adulthood. Smoking has elements of risk-taking and rebellion, which often appeal to young people. The presence of high-status models and peers may also encourage smoking. Because teenagers are influenced more by their peers than by adults, attempts by parents, schools, and health professionals at preventing people from trying cigarettes are often unsuccessful.[53][54]
Children of smoking parents are more likely to smoke than children with non-smoking parents. One study found that parental smoking cessation was associated with less adolescent smoking, except when the other parent currently smoked.[55] A current study tested the relation of adolescent smoking to rules regulating where adults are allowed to smoke in the home. Results showed that restrictive home smoking policies were associated with lower likelihood of trying smoking for both middle and high school students.[56]
Many anti-smoking organizations claim that teenagers begin their smoking habits due to peer pressure, and cultural influence portrayed by friends. However, one study found that direct pressure to smoke cigarettes did not play a significant part in adolescent smoking. In that study, adolescents also reported low levels of both normative and direct pressure to smoke cigarettes.[57] A similar study showed that individuals play a more active role in starting to smoke than has previously been acknowledged and that social processes other than peer pressure need to be taken into account.[58] Another study's results revealed that peer pressure was significantly associated with smoking behavior across all age and gender cohorts, but that intrapersonal factors were significantly more important to the smoking behavior of 12–13 year-old girls than same-age boys. Within the 14–15 year-old age group, one peer pressure variable emerged as a significantly more important predictor of girls' than boys' smoking.[59] It is debated whether peer pressure or self-selection is a greater cause of adolescent smoking. It is arguable that the reverse of peer-pressure is true, when the majority of peers do not smoke and ostracize those who do.[citation needed]
Psychologists such as Hans Eysenck have developed a personality profile for the typical smoker. Extraversion is the trait that is most associated with smoking, and smokers tend to be sociable, impulsive, risk taking, and excitement seeking individuals.[60] Although, personality and social factors may make people likely to smoke, the actual habit is a function of operant conditioning. During the early stages, smoking provides pleasurable sensations (because of its action on the dopamine system) and thus serves as a source of positive reinforcement. After an individual has smoked for many years, the avoidance of withdrawal symptoms and negative reinforcement become the key motivations.[citation needed]
Persistence
Because they are engaging in an activity that has negative effects on health, people who smoke tend to rationalize their behavior. In other words, they develop convincing, if not necessarily logical reasons why smoking is acceptable for them to do. For example, a smoker could justify his or her behavior by concluding that everyone dies and so cigarettes do not actually change anything. Or a person could believe that smoking relieves stress or has other benefits that justify its risks. These types of beliefs prevent anxiety and keep people smoking.[citation needed]
The reasons given by smokers for this activity are broadly categorized as addictive smoking, pleasure from smoking, tension reduction/relaxation, social smoking, stimulation, habit/automatism, and handling. There are gender differences in how much each of these reasons contribute, with females more likely than males to cite tension reduction/relaxation, stimulation and social smoking.[61]
Some smokers argue that the depressant effect of smoking allows them to calm their nerves, often allowing for increased concentration. However, according to the Imperial College London, "Nicotine seems to provide both a stimulant and a depressant effect, and it is likely that the effect it has at any time is determined by the mood of the user, the environment and the circumstances of use. Studies have suggested that low doses have a depressant effect, while higher doses have stimulant effect."[62] However, it is impossible to differentiate a drug effect brought on by nicotine use, and the alleviation of nicotine withdrawal.[citation needed]
The lack of deterrence by the deleterious health effects is a prototypical example of optimism bias. Also, other reason for this are lack of understanding of probability, the fact that the effects usually kick in at a older age, and personality traits or disorders that generally produce high-risk or self-destructive behavior.[citation needed]
Patterns
A number of studies have established that cigarette sales and smoking follow distinct time-related patterns. For example, cigarette sales in the United States of America have been shown to follow a strongly seasonal pattern, with the high months being the months of summer, and the low months being the winter months.[63]
Similarly, cigarette smoking activity has been shown to follow distinct circadian patterns during the waking day, with the high point usually occurring shortly after waking in the morning or going to sleep at night.[64]
Impact
Economic
In countries where there is a public health system, society covers the cost of medical care for smokers who become ill through in the form of increased taxes. Two arguments exist on this front, the "pro-smoking" argument suggesting that heavy smokers generally don't live long enough to develop the costly and chronic illnesses which affect the elderly, reducing society's healthcare burden. The "anti-smoking" argument suggests that the healthcare burden is increased because smokers get chronic illnesses younger and at a higher rate than the general population.
Data on both positions is limited. The Centers for Disease Control and Prevention published research in 2002 claiming that the cost of each pack of cigarettes sold in the United States was more than $7 in medical care and lost productivity.[65] The cost may be higher, with another study putting it as high as $41 per pack, most of which however is on the individual and his/her family.[66] This is how one author of that study puts it when he explains the very low cost for others: "The reason the number is low is that for private pensions, Social Security, and Medicare — the biggest factors in calculating costs to society — smoking actually saves money. Smokers die at a younger age and don't draw on the funds they've paid into those systems."[66]
By contrast, some non-scientific studies, including one conducted by Philip Morris in the Czech Republic[67] and another by the Cato Institute,[68] support the opposite position. Neither study was peer-reviewed nor published in a scientific journal, and the Cato Institute has received funding from tobacco companies in the past.[citation needed] Philip Morris has explicitly apologised for the former study, saying: "The funding and public release of this study which, among other things, detailed purported cost savings to the Czech Republic due to premature deaths of smokers, exhibited terrible judgment as well as a complete and unacceptable disregard of basic human values. For one of our tobacco companies to commission this study was not just a terrible mistake, it was wrong. All of us at Philip Morris, no matter where we work, are extremely sorry for this. No one benefits from the very real, serious and significant diseases caused by smoking." [67]
Between 1970 an 1995, per-capita cigarette consumption in poorer developing countries increased by 67 percent, while it dropped by 10 percent in the richer developed world. Eighty percent of smokers now live in less developed countries. By 2030, the World Health Organization (WHO) forecasts that 10 million people a year will die of smoking-related illness, making it the single biggest cause of death worldwide, with the largest increase to be among women. WHO forecasts' the 21st century's death rate from smoking to be ten times the 20th century's rate. ("Washingtonian" magazine, December 2007).
Health
Fresh tobacco, processed tobacco, and tobacco smoke contain carcinogens. The current view on cancer is that carcinogenicity is a stochastic effect, where various environmental factors trigger the development of cancer. While exposure to a carcinogen increases the probability of cancer, the process remains random. For example, smoking tobacco is known to cause cancer in humans, but not all people who smoke necessarily develop smoking-related cancer. Additionally, in studies on humans, the large number of confounding variables makes it challenging to statistically distinguish their effects.
Tobacco use leads most commonly to diseases affecting the heart and lungs, with smoking being a major risk factor for heart attacks, strokes, Chronic Obstructive Pulmonary Disease (COPD), emphysema, and cancer.
Social
Famous smokers of the past used cigarettes or pipes as part of their image, such as Jean Paul Sartre's Gauloise-brand cigarettes, Albert Einstein's, Joseph Stalin's, Douglas MacArthur's, Bertrand Russell's, and Bing Crosby's pipes, or the news broadcaster Edward R. Murrow's cigarette. Writers in particular seemed to be known for smoking; see, for example, Cornell Professor Richard Klein's book Cigarettes are Sublime for the analysis, by this professor of French literature, of the role smoking plays in 19th and 20th century letters. The popular author Kurt Vonnegut addressed his addiction to cigarettes within his novels. British Prime Minister Harold Wilson was well known for smoking a pipe in public as was Winston Churchill for his cigars. Sherlock Holmes, the fictional detective created by Sir Arthur Conan Doyle smoked a pipe, cigarettes, and cigars, besides injecting himself with cocaine, "to keep his overactive brain occupied during the dull London days, when nothing happened". The DC Vertigo comic book character, John Constantine, created by Alan Moore, is synonymous with smoking, so much so that the first storyline by Preacher creator, Garth Ennis, centred around John Constantine contracting lung cancer. Professional wrestler James Fullington, while in character as "The Sandman", is a chronic smoker in order to appear "tough".
In most major religions, tobacco smoking is not specifically prohibited, although it may be discouraged as an immoral habit.
Communal smoking of a sacred tobacco pipe is a common ritual of many Native American tribes, and was considered a sacred part of their religion. Sema, the Anishinaabe word for tobacco, was grown for ceremonial use and considered the ultimate sacred plant since its smoke was believed to carry prayers to the heavens. The tobacco used during these rituals varies widely in potency — the Nicotiana rustica species used in South America, for instance, has up to twice the nicotine content of the common North American N. tabacum.
Before the health risks of smoking were identified through controlled study, smoking was considered an immoral habit by certain Christian preachers and social reformers. The founder of the Latter Day Saint movement, Joseph Smith, Jr, recorded that on February 27, 1833, he received a revelation which addressed tobacco use. Eventually accepted as a commandment, adherent Mormons do not smoke.
Jehovah's Witnesses base their stand against smoking on the Bible's command to "clean ourselves of every defilement of flesh" (2 Corinthians 7:1)
The Jewish Rabbi Yisrael Meir Kagan (1838–1933) was one of the first Jewish authorities to speak out on smoking.
In the Sikh religion, tobacco smoking is strictly forbidden.
In the Bahá'í Faith, smoking tobacco is discouraged though not forbidden.[69]
Public policy
On February 27, 2005 the WHO Framework Convention on Tobacco Control, took effect. The FCTC is the world's first public health treaty. Countries that sign on as parties agree to a set of common goals, minimum standards for tobacco control policy, and to cooperate in dealing with cross-border challenges such as cigarette smuggling. Currently the WHO declares that 4 billion people will be covered by the treaty, which includes 168 signatories.[70] Among other steps, signatories are to put together legislation that will eliminate secondhand smoke in indoor workplaces, public transport, indoor public places and, as appropriate, other public places.
Taxation
Many governments have introduced excise taxes on cigarettes in order to reduce the consumption of cigarettes. Money collected from the cigarette taxes are frequently used to pay for tobacco use prevention programs, therefore making it a method of internalizing external costs.[citation needed]
In 2002, the Centers for Disease Control and Prevention said that each pack of cigarettes sold in the United States costs the nation more than $7 in medical care and lost productivity.[65] That's over $2000 per year/smoker. Another study by a team of health economists finds the combined price paid by their families and society is about $41 per pack of cigarettes.[71]
Substantial scientific evidence shows that higher cigarette prices result in lower overall cigarette consumption. Most studies indicate that a 10% increase in price will reduce overall cigarette consumption by 3% to 5%. Youth, minorities, and low-income smokers are two to three times more likely to quit or smoke less than other smokers in response to price increases.[72][73] Smoking is often cited as an example of an inelastic good, however, i.e. a large rise in price will only result in a small decrease in consumption.
Many nations have implemented some form of tobacco taxation. As of 1997, Denmark had the highest cigarette tax burden of $4.02 per pack. Taiwan only had a tax burden of $0.62 per pack. Currently, the average price and excise tax on cigarettes in the United States is well below those in many other industrialized nations.[74]
Cigarette taxes vary widely from state to state in the United States. For example, South Carolina has a cigarette tax of only 7 cents per pack, the nation's lowest, while New Jersey has the highest cigarette tax in the U.S.: $2.575 per pack. In Alabama, Illinois, Missouri, New York City, Tennessee, and Virginia, counties and cities may impose an additional limited tax on the price of cigarettes.[75] Due to the high tax rate, the price of an average pack of cigarettes in New Jersey is $6.45,[76][77] which is still less than the approximated external cost of a pack of cigarettes.
In Canada, cigarette taxes have raised prices of the more expensive brands to upwards of ten CAD$.
In the United Kingdom, a packet of cigarettes typically costs between £4.25 and £5.50 depending on the brand purchased and where the purchase was made.[78] The UK has a strong black market for cigarettes which has formed as a result of the high taxation, and it is estimated 27% of cigarette and 68% of handrolling tobacco consumption was non-UK duty paid (NUKDP).[79]
Restrictions
In June 1967, the Federal Communications Commission ruled that programs broadcast on a television station that discussed smoking and health were insufficient to offset the effects of paid advertisements that were broadcast for five to ten minutes each day.In April 1970, Congress passed the Public Health Cigarette Smoking Act banning the advertising of cigarettes on television and radio starting on January 2, 1971.[80]
The Tobacco Advertising Prohibition Act 1992 expressly prohibited almost all forms of Tobacco advertising in Australia, including the sponsorship of sporting or other cultural events by cigarette brands.
All tobacco advertising and sponsorship on television has been banned within the European Union since 1991 under the Television Without Frontiers Directive (1989)[81] This ban was extended by the Tobacco Advertising Directive, which took effect in July 2005 to cover other forms of media such as the internet, print media, and radio. The directive does not include advertising in cinemas and on billboards or using merchandising – or tobacco sponsorship of cultural and sporting events which are purely local, with participants coming from only one Member State[82] as these fall outside the jurisdiction of the European Commission. However, most member states have transposed the directive with national laws that are wider in scope than the directive and cover local advertising. A 2008 European Commission report concluded that the directive had been successfully transposed into national law in all EU member states, and that these laws were well implemented.[83]
Some countries also impose legal requirements on the packaging of tobacco products. For example in the countries of the European Union, Turkey, Australia[84] and South Africa, cigarette packs must be prominently labeled with the health risks associated with smoking.[85] Canada, Australia, Thailand, Iceland and Brazil have also imposed labels upon cigarette packs warning smokers of the effects, and they include graphic images of the potential health effects of smoking. Cards are also inserted into cigarette packs in Canada. There are sixteen of them, and only one comes in a pack. They explain different methods of quitting smoking. Also, in the United Kingdom, there have been a number of graphic NHS advertisements, one showing a cigarette filled with fatty deposits, as if the cigarette is symbolising the artery of a smoker.
Many countries have a smoking age, In many countries, including the United States, most European Union member states, New Zealand, Canada, South Africa, Israel, India, Brazil, Chile, Costa Rica and Australia, it is illegal to sell tobacco products to minors and in the Netherlands, Austria, Belgium, Denmark and South Africa it is illegal to sell tobacco products to people under the age of 16. On September 1, 2007 the minimum age to buy tobacco products in Germany rose from 16 to 18, as well as in Great Britain where on October 1, 2007 it rose from 16 to 18.[86] In 46 of the 50 United States, the minimum age is 18, except for Alabama, Alaska, New Jersey, and Utah where the legal age is 19 (also in Onondaga County in upstate New York, as well as Suffolk and Nassau Counties of Long Island, New York).[citation needed] Some countries have also legislated against giving tobacco products to (i.e. buying for) minors, and even against minors engaging in the act of smoking.[citation needed] Underlying such laws is the belief that people should make an informed decision regarding the risks of tobacco use. These laws have a lax enforcement in some nations and states. In other regions, cigarettes are still sold to minors because the fines for the violation are lower or comparable to the profit made from the sales to minors.[citation needed] However in China, Turkey, and many other countries usually a child will have little problem buying tobacco products, because they are often told to go to the store to buy tobacco for their parents.
Several countries such as the Ireland, Latvia, Estonia, The Netherlands, France, Finland, Norway, Canada, Australia, Sweden, Portugal, Singapore, Italy, Indonesia, India, Lithuania, Chile, Spain, Iceland, United Kingdom, Slovenia and Malta have legislated against smoking in public places, often including bars and restaurants. Restaurateurs have been permitted in some jurisdictions to build designated smoking areas (or to prohibit smoking). In the United States, many states prohibit smoking in restaurants, and some also prohibit smoking in bars. In provinces of Canada, smoking is illegal in indoor workplaces and public places, including bars and restaurants. As of March 31, 2008 Canada has introduced a smoking ban in all public places, as well as within 10 meters of an entrance to any public place. In Australia, smoking bans vary from state to state. Currently, Queensland has total bans within all public interiors (including workplaces, bars, pubs and eateries) as well as patrolled beaches and some outdoor public areas. There are, however, exceptions for designated smoking areas. In Victoria, smoking is banned in train stations, bus stops and tram stops as these are public locations where second hand smoke can affect non-smokers waiting for public transport, and since July 1, 2007 is now extended to all indoor public places. In New Zealand and Brazil, smoking is banned in enclosed public places mainly bars, restaurants and pubs. Hong Kong banned smoking on January 1, 2007 in the workplace, public spaces such as restaurants, karaoke rooms, buildings, and public parks. Bars serving alcohol who do not admit under-18s have been exempted till 2009. In Romania smoking is illegal in trains, metro stations, public institutions (except where designated, usually outside) and public transportation.
Product safety
An indirect public health problem posed by cigarettes is that of accidental fires, usually linked with consumption of alcohol. Numerous cigarette designs have been proposed, some by tobacco companies themselves, which would extinguish a cigarette left unattended for more than a minute or two, thereby reducing the risk of fire. Among American tobacco companies, some have resisted this idea, while others have embraced it. RJR Reynolds was a leader in making prototypes of these cigarettes in 1983[87] and will make all of their U.S. market cigarettes to be fire-safe by 2010.[88] Phillip Morris is not in active support of it.[89] Lorillard, the nation's third largest tobacco company, seems to be ambivalent.[89]
Gateway drug theory
The relationship between tobacco and other drug use has been well-established, however the nature of this association remains unclear. The two main theories are the phenotypic causation (gateway) model and the correlated liabilities model. The causation model argues that smoking is a primary influence on future drug use,[90] while the correlated liabilities model argues that smoking and other drug use are predicated on genetic or environmental factors.[91]
Cessation
Smoking cessation, referred to as "quitting" is the action leading towards abstinence of tobacco smoking. There are a number of methods such as cold turkey, nicotine replacement therapy, antidepressants, hypnosis, self-help, and support groups.
Gallery
![]() Textbooks from Wikibooks
Textbooks from Wikibooks
![]() Quotations from Wikiquote
Quotations from Wikiquote
![]() Source texts from Wikisource
Source texts from Wikisource
![]() Images and media from Commons
Images and media from Commons
![]() News stories from Wikinews
News stories from Wikinews
|




References
Notes
- ^ a b Gately, Iain (2004) [2003], Tobacco: A Cultural History of How an Exotic Plant Seduced Civilization, Diane, ISBN 0-80213-960-4
- ^ a b Wilbert, Johannes (1993-07-28), Tobacco and Shamanism in South America, Yale University Press, ISBN 0300057903, http://books.google.com/books?id=qPCuo4LkrIwC&printsec=frontcover&dq=Tobacco+and+Shamanism+in+South+America, retrieved on 2009-03-22
- ^ a b Robicsek, Francis (January 1979), The Smoking Gods: Tobacco in Maya Art, History, and Religion, University of Oklahoma Press, p. 30, ISBN 0806115114
- ^ a b c Lloyd, John; Mitchinson, John (2008-07-25), The Book of General Ignorance, Harmony Books, ISBN 0307394913
- ^ a b c Proctor 2000, p. 228
- ^ a b Doll Richard, Bradford Hilly A (June 26, 1954). "The mortality of doctors in relation to their smoking habits. A preliminary report". British Medical Journal 328 (4877): 1451–55. doi:. PMID 13160495. http://bmj.bmjjournals.com/cgi/reprint/328/7455/1529.
- ^ a b VJ Rock, MPH, A Malarcher, PhD, JW Kahende, PhD, K Asman, MSPH, C Husten, MD, R Caraballo, PhD (2007-11-09). "Cigarette Smoking Among Adults --- United States, 2006". United States Centers for Disease Control and Prevention. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5644a2.htm. Retrieved on 2009-01-01. "[...]In 2006, an estimated 20.8% (45.3 million) of U.S. adults[...]"
- ^ a b c d e "WHO/WPRO-Smoking Statistics". World Health Organization Regional Office for the Western Pacific. 2002-05-28. http://www.wpro.who.int/media_centre/fact_sheets/fs_20020528.htm. Retrieved on 2009-01-01.
- ^ a b c Wingand, Jeffrey S. (July 2006). "ADDITIVES, CIGARETTE DESIGN and TOBACCO PRODUCT REGULATION". written at Mt. Pleasant, MI 48804 (PDF). Jeffrey Wigand. http://www.jeffreywigand.com/WHOFinal.pdf. Retrieved on 2009-02-14.
- ^ a b Gilman & Xun 2004, p. 318
- ^ a b Parrott, A. C.; Winder, G. (1989-02). "Nicotine chewing gum (2 mg, 4 mg) and cigarette smoking: comparative effects upon vigilance and heart rate". Psychopharmacology (Berlin: Springer) 97 (2): 257. doi:. PMID 2498936. http://www.springerlink.com/content/v2275360j2r26051/. Retrieved on 2009-03-22.
- ^ a b Wesnes, K.; Warburton, D.M. (1997-09-22). "The effects of cigarette smoking on overnight performance". Psychopharmacology (Department of Psychology, University of Reading, England: Springer Berlin) 136 (2): 172. doi:. http://www.springerlink.com/content/f6gxhlj63peeytlr/. Retrieved on 2009-03-21.
- ^ a b Gilman & Xun 2004, pp. 320–321
- ^ a b c Guindon, G. Emmanuel; Boisclair, David (2003) (PDF), Past, current and future trends in tobacco use, Washington DC: The International Bank for Reconstruction and Development / The World Bank, pp. 13–16, http://www1.worldbank.org/tobacco/pdf/Guindon-Past,%20current-%20whole.pdf, retrieved on 2009-03-22
- ^ a b The World Health Organization, and the Institute for Global Tobacco Control, Johns Hopkins School of Public Health (2001). "Women and the Tobacco Epidemic: Challenges for the 21st Century". World Health Organization. 5-6. http://www.who.int/tobacco/media/en/WomenMonograph.pdf. Retrieved on 2009-01-02.
- ^ a b "Surgeon General's Report—Women and Smoking". Centers for Disease Control and Prevention. 2001. 47. http://www.cdc.gov/tobacco/data_statistics/sgr/sgr_2001/sgr_women_chapters.htm. Retrieved on 2009-01-03.
- ^ Heckewelder, John Gottlieb Ernestus; Reichel, William Cornelius (June 1971) [1876], History, manners, and customs of the Indian nations who once inhabited Pennsylvania and the neighbouring states, The Historical society of Pennsylvania, p. 149, ISBN 978-0405028533, http://books.google.com/books?id=F8wLAAAAYAAJ&dq=History,+Manners+and+Customs+of+the+Indian+Nations+who+Once+Inhabited+Pennsylvania&printsec=frontcover&source=bl&ots=3_93XnXaGk&sig=kASn2_XGtntznuvV0kTA-T5mLgs&hl=en&ei=bRLGSbSKDp3gsAPW7536Bg&sa=X&oi=book_result&resnum=1&ct=result#PPA149,M1, retrieved on 2009-03-22
- ^ Diéreville; Webster, John Clarence; Webster, Alice de Kessler Lusk (1933), Relation of the voyage to Port Royal in Acadia or New France, The Champlain Society, "They smoke with excessive eagerness [...] men, women, girls and boys, all find their keenest pleasure in this way"
- ^ Gottsegen, Jack Jacob (1940) Tobacco: A Study of Its Consumption in the United StatesPitman Publishing Companyp. 107 http://books.google.com/books?id=1uNCAAAAIAAJ&q=Tobacco:+A+Study+of+Its+Consumption+in+the+United+States&dq=Tobacco:+A+Study+of+Its+Consumption+in+the+United+States&pgis=1. Retrieved on 2009-03-22
- ^ Balls, Edward K. (1962-10-01), Early Uses of California Plants, University of California Press, pp. 81–85, ISBN 978-0520000728, http://books.google.com/books?id=F2RzddT6xAsC&printsec=frontcover&dq=Early+Uses+of+California+Plants, retrieved on 2009-03-22
- ^ Jordan, Jr., Ervin L., Jamestown, Virginia, 1607-1907: An Overview, University of Virginia, http://curry.edschool.virginia.edu/socialstudies/projects/jvc/overview.html, retrieved on 2009-02-22
- ^ Kulikoff, Allan (1986-08-01), Tobacco and Slaves: The Development of Southern Cultures in the Chesapeake, The University of North Carolina Press, ISBN 978-0807842249, http://books.google.com/books?id=NCvU9_bj-1QC&printsec=frontcover&dq=Tobacco+%26+Slaves:+The+Development+of+Southern+Cultures+in+the+Chesapeake, retrieved on 2009-03-22
- ^ Cooper, William James (October 2000), Liberty and Slavery: Southern Politics to 1860, Univ of South Carolina Press, p. 9, ISBN 978-1570033872, http://books.google.com/books?id=AFS3Uu_EMQEC&printsec=frontcover#PPA9,M1, retrieved on 2009-03-22
- ^ Trager, James (August 1994), The People's Chronology: A Year-by-year Record of Human Events from Prehistory to the Present, Holt, ISBN 978-0805031348
- ^ Gilman & Xun 2004, p. 38
- ^ Gilman & Xun 2004, pp. 92-99
- ^ Gilman & Xun 2004, pp. 15-16
- ^ A Counterblaste to Tobacco, University of Texas at Austin, 2002-04-16, http://www.laits.utexas.edu/poltheory/james/blaste/, retrieved on 2009-03-22
- ^ Burns, Eric (2006-09-28), The Smoke of the Gods: A Social History of Tobacco, Temple University Press, pp. 134–135, ISBN 978-1592134809, http://books.google.com/books?id=cZfqS7vi9vEC&printsec=frontcover&dq=The+Smoke+of+the+Gods:+A+Social+History+of+Tobacco, retrieved on 2009-03-22
- ^ Proctor 2000, p. 178
- ^ Proctor 2000, p. 219
- ^ Proctor 2000, p. 187
- ^ a b Proctor 2000, p. 245
- ^ Proctor, Robert N. (1996), Nazi Medicine and Public Health Policy, Dimensions, Anti-Defamation League, http://www.adl.org/Braun/dim_14_1_nazi_med.asp, retrieved on 2008-06-01
- ^ Doll, Rich; and Hilly, A. Bradford (September 30, 1950). "Smoking and carcinoma of the lung. Preliminary report". British Medical Journal 2 (4682): 739–48. PMID 14772469.
- ^ Milo Geyelin (November 23, 1998). "Forty-Six States Agree to Accept $206 Billion Tobacco Settlement". Wall Street Journal.
- ^ Hilton, Matthew (2000-05-04), Smoking in British Popular Culture, 1800-2000: Perfect Pleasures, Manchester University Press, pp. 229–241, ISBN 978-0719052576, http://books.google.com/books?id=UjM8t6Ul73YC&printsec=frontcover&dq=Smoking+in+British+Popular+Culture#PPA229,M1, retrieved on 2009-03-22
- ^ Gilman & Xun 2004, pp. 46-57
- ^ WHO REPORT on the global TOBACCO epidemic 2008, pp. 267–288
- ^ "Bidi Use Among Urban Youth -- Massachusetts, March-April 1999". Centers for Disease Control and Prevention. 1999-09-17. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4836a2.htm. Retrieved on 2009-02-14.
- ^ Pakhale SS, Maru GB. (1998-12-12). Distribution of major and minor alkaloids in tobacco, mainstream and sidestream smoke of popular Indian smoking products. Parel, Mumbai, India: Tata Memorial Centre. PMID 9862656.
- ^ Rarick CA (2008-04-02). Note on the premium cigar industry. SSRN. http://ssrn.com/abstract=1127582. Retrieved on 2008-12-02.
- ^ Mariolis P, Rock VJ, Asman K et al. (2006). "Tobacco use among adults—United States, 2005". MMWR Morb Mortal Wkly Rep 55 (42): 1145–8. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5542a1.htm.
- ^ Library of Congress (2004-05-20). A bill to protect the public health by providing the Food and Drug Administration with certain authority to regulate tobacco products. (Summary). Press release. http://thomas.loc.gov/cgi-bin/bdquery/z?d108:SN02461:@@@D&summ2=m&. Retrieved on 2007-08-01.
- ^ Wonnacott, S (1997-02). "Presynaptic nicotinic ACh receptors". Trends in neurosciences 20 (2): 92–8. doi:. PMID 9023878. http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6T0V-3P6B0H6-1J&_user=10&_rdoc=1&_fmt=&_orig=search&_sort=d&view=c&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=824dbe9fbdcdbfd9e67f659ceaf92343.
- ^ Talhout R, Opperhuizen A, van Amsterdam JG (October 2007). "Role of acetaldehyde in tobacco smoke addiction". Eur Neuropsychopharmacol 17 (10): 627–36. doi:. PMID 17382522.
- ^ WHO REPORT on the global TOBACCO epidemic 2008, pp. 267–288
- ^ Peto, Richard; Lopez, Alan D; Boreham, Jillian; Thun, Michael (2006) (PDF), Mortality from Smoking in Developed Countries 1950-2000: indirect estimates from national vital statistics, Oxford University Press, p. 9, http://www.ctsu.ox.ac.uk/~tobacco/SMK_All_PAGES.pdf, retrieved on 2009-03-22
- ^ VJ Rock, MPH, A Malarcher, PhD, JW Kahende, PhD, K Asman, MSPH, C Husten, MD, R Caraballo, PhD (2007-11-09). "Cigarette Smoking Among Adults --- United States, 2006". United States Centers for Disease Control and Prevention. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5644a2.htm. Retrieved on 2009-01-01. "[...]In 2006, an estimated 20.8% (45.3 million) of U.S. adults[...]"
- ^ The Global Burden of Disease 2004 Update 2008, p. 8
- ^ The Global Burden of Disease 2004 Update 2008, p. 23
- ^ a b "WHO/WPRO-Tobacco Fact sheet". World Health Organization Regional Office for the Western Pacific. 2007-05-29. http://www.wpro.who.int/media_centre/fact_sheets/fs_20070529.htm. Retrieved on 2009-01-01.
- ^ Silva, Phil A. (1992). "A longitudinal study of the influence of parents and friends on children's initiation of smoking". Journal of Applied Developmental Psychology (New Zealand: University of Otago Medical School) 13 (4): 423. doi:. http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6W52-46H16G4-8F&_user=10&_coverDate=12/31/1992&_rdoc=1&_fmt=high&_orig=browse&_srch=doc-info(%23toc%236558%231992%23999869995%23332094%23FLP%23display%23Volume)&_cdi=6558&_sort=d&_docanchor=&_ct=10&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=c8c5d19384eb048e0bdbb30844f72706. Retrieved on 2009-03-22.
- ^ Harris, Judith Rich; Pinker, Steven (1998-09-04), The nurture assumption: why children turn out the way they do, Simon and Schuster, ISBN 978-0684844091, http://books.google.com/books?id=9GQlA_l-TQ0C&printsec=frontcover&dq=The+nurture+assumption:+Why+children+turn+out+the+way+they+do, retrieved on 2009-03-22
- ^ Chassin L, Presson C, Rose J, Sherman SJ, Prost J (September 2002). "Parental smoking cessation and adolescent smoking". J Pediatr Psychol 27 (6): 485–96. doi:. PMID 12177249. http://jpepsy.oxfordjournals.org/cgi/content/abstract/27/6/485.
- ^ Proescholdbell RJ, Chassin L, MacKinnon DP (May 2000). "Home smoking restrictions and adolescent smoking". Nicotine Tob Res. 2 (2): 159–67. doi:. PMID 11072454.
- ^ Urberg KA, Shyu SJ, Liang J (1990). "Peer influence in adolescent cigarette smoking". Addict Behav 15 (3): 247–55. doi:. PMID 2378284.
- ^ Michell L, West P (1996). Peer pressure to smoke: the meaning depends on the method. 11. pp. 39–49. http://www.oxfordjournals.org/our_journals/healed/online/Volume_11/Issue_01/110039.sgm.abs.html.
- ^ Barber JG, Bolitho F, Bertrand LD (1999). "The predictors of adolescent smoking". Journal of Social Service Research 26 (1): 51–66. doi:.
- ^ Eysenck, Hans J.; Brody, Stuart (2000-11), Smoking, health and personality, Transaction, ISBN 978-0765806390, http://books.google.com/books?id=&printsec=frontcover&dq=Smoking,+health+and+personality, retrieved on 2009-03-22
- ^ Berlin, Ivan; Edward G. Singleton; Anne-Marie Pedarriosse; Sylvie Lancrenon; Alexis Rames; Henri-Jean Aubin; Raymond Niaura (2003-11). "The Modified Reasons for Smoking Scale: factorial structure, gender effects and relationship with nicotine dependence and smoking cessation in French smokers". Addiction 98 (11): 1575–83. doi:. http://www.ingentaconnect.com/content/bsc/add/2003/00000098/00000011/art00013.
- ^ Nicotine, Imperial College London, http://www.ch.ic.ac.uk/rzepa/mim/drugs/html/nicotine_text.htm, retrieved on 2009-03-22
- ^ Chandra S, Chaloupka FJ (March 2003). "Seasonality in cigarette sales: patterns and implications for tobacco control". Tob Control 12 (1): 105–7. doi:. PMID 12612375. PMC: 1759100. http://tobaccocontrol.bmj.com/cgi/content/extract/12/1/105.
- ^ Chandra S, Shiffman S, Scharf DM, Dang Q, Shadel WG (February 2007). "Daily smoking patterns, their determinants, and implications for quitting". Exp Clin Psychopharmacol 15 (1): 67–80. doi:. PMID 17295586. http://psycnet.apa.org/journals/pha/15/1/67/.
- ^ a b Cigarettes Cost U.S. $7 Per Pack Sold, Study Says
- ^ a b Study: Cigarettes cost families, society $41 per pack
- ^ a b "Public Finance Balance of Smoking in the Czech Republic". http://www.mindfully.org/Industry/Philip-Morris-Czech-Study.htm.
- ^ "Snuff the Facts". http://www.cato.org/dailys/1-16-98.html.
- ^ Smith, Peter (2000). "smoking". A concise encyclopedia of the Bahá'í Faith. Oxford: Oneworld Publications. pp. p. 323. ISBN 1-85168-184-1.
- ^ Updated status of the WHO Framework Convention on Tobacco Control
- ^ 26, 2004-smoking-costs_x.htm Study: Cigarettes cost families, society $41 per pack
- ^ Reducing Tobacco Use: A Report of The Surgeon General
- ^ Higher cigarette prices influence cigarette purchase patterns
- ^ Cigarette Tax Burden - U.S. & International - IPRC
- ^ State Tax Rates on Cigarettes
- ^ N.J. cigarette tax increase falls short for Cancer Society
- ^ Campaign for Tobacco-Free Kids factsheet showing breakdown of costs by state
- ^ Price of cigarettes across the EU
- ^ Smuggling & Crossborder Shopping
- ^ History of Tobacco Regulation
- ^ Television Without Frontiers Directive 1989
- ^ European Union - Tobacco advertising ban takes effect 31 July 
- ^ Report on the implementation of the EU Tobacco Advertising Directive
- ^ Tobacco - Health warnings Australian Government Department of Health and Ageing. Retrieved August 29, 2008
- ^ Public Health at a Glance - Tobacco Pack Information
- ^ Tobacco 18
- ^ NFPA :: Press Room :: News releases
- ^ Reynolds Letter
- ^ a b Fire Safe Cigarettes :: Letter to tobacco companies
- ^ Merrill, Jeffrey C.; Kleber, Herbert D.; Shwartz, Michael; Liu, Hong; Lewis, Susan R. (1999-10-01). "Cigarettes, alcohol, marijuana, other risk behaviors, and American youth". Drug Alcohol Depend (Philadelphia, PA 19103, USA: Economic and Policy Research, Treatment Research Institute) 56 (3): 205. doi:. PMID 10529022. http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6T63-3X941H9-4&_user=10&_rdoc=1&_fmt=&_orig=search&_sort=d&view=c&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=2c6497433ff41875353e9b99d0e5748a. Retrieved on 2009-03-22.
- ^ Swan, GE; Carmelli, D; Rosenman, RH; Fabsitz, RR; Christian, JC (1990). "Smoking and alcohol consumption in adult male twins: genetic heritability and shared environmental influences". Substance Abuse 2 (1). PMID 2136102.
Bibliography
- Gilman, Sander L.; Xun, Zhou (2004-08-15), Smoke: A Global History of Smoking, Reaktion Books, ISBN 978-1861892003, http://books.google.com/books?id=mM5bYb_uVcwC&printsec=frontcover&dq=smoke, retrieved on 2009-03-22
- Proctor, Robert N. (2000-11-15), The Nazi War on Cancer, Princeton University Press, ISBN 978-0691070513, http://books.google.com/books?id=02NGyKTwko0C&printsec=frontcover&dq=The+Nazi+War+on+Cancer, retrieved on 2009-03-22
- "The Global Burden of Disease 2004 Update". World Health Organization. 2008. http://www.who.int/entity/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Retrieved on 2008-01-01.
- "WHO REPORT on the global TOBACCO epidemic". World Health Organization. 2008. http://www.who.int/entity/tobacco/mpower/mpower_report_full_2008.pdf. Retrieved on 2008-01-01.

